Browse our range of reports and publications including performance and financial statement audit reports, assurance review reports, information reports and annual reports.
Auditor-General Report No. 33 of 2014–15
Organ and Tissue Donation: Community Awareness, Professional Education and Family Support
Published
Wednesday 29 April 2015

Portfolio
Health
Entity
Australian Organ and Tissue Donation and Transplantation Authority
Contact
Please direct enquiries relating to reports through our contact page.
Sector
Health
The audit objective was to assess the effectiveness of the Australian Organ and Tissue Donation and Transplantation Authority's administration of community awareness, professional education and donor family support activities intended to increase organ an
Summary
Introduction
1. The Australian organ and tissue donation system is based on an ‘informed consent’ (or opt-in) model, whereby individuals agree to donate their organs and tissue in the event of their death.1 Individuals can record their consent or objection to becoming an organ and/or tissue donor on the Australian Organ Donor Register (AODR).2 Regardless of whether an individual has registered their consent for donation, the practice in Australia is to also seek agreement from a donor’s next of kin before donation proceeds.3
2. Australia’s rate of organ and tissue donation does not meet the current demand for transplantation. In 2014, an average of 1632 people were on organ transplant waiting lists each month, and in total, 1117 people received organ transplants. In the same year, 5553 people received tissue transplants.
3. In October 2006, the then Australian Government established the National Clinical Taskforce on Organ and Tissue Donation (the Taskforce) to provide evidence-based advice on ways to increase the rate of organ and tissue donation.4 In response to the Taskforce report, the Australian Government announced in July 2008 a national reform program to ‘establish Australia as a world leader in organ donation for transplantation’.5 Endorsed by the Council of Australian Governments (COAG), the national reform program committed $136.4 million in new Australian Government funding over four years (2008–2012) to improve access to transplants through a nationally coordinated approach to organ and tissue donation.
4. The national reform program had two objectives: to increase the capability and capacity within the health system to maximise donation rates; and raise community awareness and stakeholder engagement across Australia to promote organ and tissue donation. Nine measures were endorsed by COAG aimed at achieving the two broad program objectives:
- Measure 1: A new national approach and system – a national authority6 and network of organ procurement organisations.
- Measure 2: Specialist hospital staff and systems dedicated to organ donation.
- Measure 3: New funding for hospitals.
- Measure 4: National professional awareness and education.
- Measure 5: Coordinated ongoing community awareness and education.
- Measure 6: Support for donor families.
- Measure 7: Safe, equitable and transparent national transplantation process.
- Measure 8: National eye and tissue donation and transplantation.
- Measure 9: Additional national initiatives, including living donation programs.
5. This audit focussed on Measures 4 to 6 highlighted above, relating to: professional education; community awareness; and support for donor families.
6. Measure 1 of the national reform program included establishing the Australian Organ and Tissue Donation and Transplantation Authority (OTA) in January 2009, as well as establishing DonateLife Agencies in each state to manage the donation process at the state level.7 OTA has overall national responsibility for the implementation of the nine COAG reform measures, working in collaboration with state and territory (state) based DonateLife8 Agencies.
7. OTA administers Australian Government funding to each state government to employ DonateLife staff in 72 hospitals9 and eight DonateLife Agencies; which together with OTA comprise the DonateLife Network. At the end of June 2014, the DonateLife Network included: 175 hospital-based medical and nursing specialists in organ and tissue donation; and 100 staff (principally specialist nurses) in the eight DonateLife Agencies.
Audit objective and scope
8. The audit objective was to assess the effectiveness of OTA’s administration of community awareness, professional education and donor family support activities intended to increase organ and tissue donation.
9. The high-level criteria developed to assist in evaluating OTA’s performance relating to the administration of the community awareness, professional education and donor family support activities were that OTA:
- plans and designs targeted activities;
- effectively administers activities in accordance with relevant frameworks10; and
- assesses and reports on the effectiveness of activities.
10. The audit scope included an assessment of OTA’s role in delivering Measures 4, 5 and 6 of the national reform program. For Measure 4, the audit focussed on OTA’s Professional Education Package. The audit did not assess: the six remaining measures; the Department of Human Services’ administration of the Australian Organ Donor Register (AODR); or state and territory responsibilities under the national reform program.
Overall conclusion
11. The Australian Organ and Tissue Donation and Transplantation Authority (OTA) is responsible for leading the implementation of the national reform program for organ and tissue donation, endorsed by COAG in 2008. The reform program comprises nine measures intended to introduce a nationally consistent approach for organ and tissue donation within a sector which has historically been state-based, and its successful implementation requires collaboration and consultation between OTA and key government and non-government stakeholders. The focus of this audit was on the measures relating to: professional awareness and education (Measure 4); coordinated and ongoing community awareness and education (Measure 5); and support for donor families (Measure 6).
12. Overall, OTA has made reasonable progress in implementing Measures 4, 5 and 6 of the national reform program, including the introduction of a Professional Education Package and National Donor Family Support Service (NDFSS). OTA has also undertaken a range of initiatives aimed at increasing community awareness and education about organ and tissue donation and transplantation. Of particular note is OTA’s approach to engaging with culturally and linguistically diverse (CALD) communities, which has been consultative and informed by relevant research. Similarly, OTA adopted an evidence-based approach to selecting the key message for its $13.8 million national advertising campaign conducted from 2010 to 2012, which tracking research indicated achieved good outcomes against campaign benchmarks in its first phase. However, a key shortcoming across the three reform measures examined in this audit was the absence of suitable performance indicators and related targets to help assess the effectiveness of initiatives. Further, in relation to Measures 5 and 6, the audit identified opportunities for OTA to: more actively facilitate collaboration among key stakeholders; improve the transparency of its grants administration; and improve the consistency of support provided to donor families.
13. Under Measure 4 (Professional awareness and education), OTA introduced a Professional Education Package (the Package) in 2012. The Package incorporated an existing training program, the Australasian Donor Awareness Program11, as well as new Family Donation Conversation (FDC) Workshops. Since the introduction of the Package, there have been over 2000 training participants. At the time of the audit, the Package was being revised, and there would be benefit in OTA continuing to monitor the ongoing effectiveness and reach of the Package by introducing relevant internal performance indicators. OTA can also improve the consistency of the application of the FDC training by confirming which family consent request model should be adopted nationally, and promoting the application of this model through the FDC Workshops.
14. As part of its implementation of Measure 5 (Community awareness and education), OTA introduced a National Community Awareness and Education Program. The program aims to promote the principles of a nationally consistent and coordinated approach within the organ and tissue donation sector to community awareness and education. While there has been a high take-up of these principles among key community organisation stakeholders, there is scope for OTA to more actively facilitate collaboration between stakeholders so as to extend the reach of community awareness and education activities. The largest financial component of the National Community Awareness and Education Program was an advertising campaign conducted by OTA. Tracking research indicated that Phase 1 of the campaign (at a cost of $9.2 million) achieved improved outcomes against the campaign benchmarks, while Phase 2 (at a cost of $4.6 million) delivered a more marginal return on investment, serving largely to help maintain the outcomes of Phase 1.
15. OTA has also introduced a range of activities and resources as part of the National Community Awareness and Education Program, including the Community Awareness Grants program which distributes approximately $500 000 per annum to grant recipients for community awareness and education activities. However, OTA’s grants guidelines do not fully outline its grants assessment process, and the ANAO identified an application which was not funded as part of a competitive grant round, but which received funding from OTA as part of an unsolicited application process. OTA can improve the transparency and equity of its granting activity by reviewing its grants administration and in particular, informing potential grant funding applicants of all sources of available grant funding and the assessment process applying to these sources.
16. As part of its implementation of Measure 6 (Support for donor families) of the national reform program, OTA introduced the National Donor Family Support Service (NDFSS) in 2011, an initiative which included revised donor family support materials and funding to the states for Donor Family Support Coordinators (DFSCs). A national study of donor family experiences during 2010 and 2011, commissioned by OTA and released in 2014, indicates that there is scope to improve the level of support for donor families, both in the hospital setting and after a donation has occurred. The introduction of specific internal performance measures would help OTA assess effectiveness and provide greater assurance that donor families are receiving consistent levels of support across Australia.
17. The ANAO has made three recommendations aimed at: improving stakeholder engagement; reviewing OTA’s grants administration; and improving donor family support services.
Key findings by chapter
Professional Education (Chapter 2)
18. Measure 4 of the national reform program required OTA to coordinate an ongoing, nationally consistent and targeted program of professional development and training for clinicians and care workers involved in organ and tissue donation. To this end, OTA introduced the Professional Education Package (the Package) in 2012 which incorporated an existing training program, the Australasian Donor Awareness Program, and two new workshops, a core and practical Family Donation Conversation (FDC) Workshop.12
19. To develop the FDC training, OTA first engaged an Australian training provider in April 2011. Participant feedback on the pilot training delivered by the provider in October 2011 indicated that it did not adequately reflect a clinical environment and consequently did not fully meet OTA’s requirements. Consequently, the training materials were revised by DonateLife clinical subject experts in 2011–12 to become the practical FDC Workshop, introduced in 2012.
20. In June 2011, OTA also engaged a United States training provider, the Gift of Life Institute, which OTA advised was the only known organisation with experience in specific organ donation consent request training. The Institute was required to revise and deliver its consent request training. This training became the core FDC Workshop and was first delivered in March 2012—one year after the planned delivery for the FDC training. Since its introduction, the workshop has been revised based on feedback from participants, as well as professional bodies.
21. In response to a decline in the number of deceased organ donors in 2014, OTA advised the Senate Community Affairs Legislation Committee in February 2015 that there was a clear difference in family consent outcomes when a trained requestor discussed organ donation with families and when an intensivist13 discussed donation with families. OTA acknowledged that it needed to reinforce its expectation that relevant staff undertake the FDC training and adopt the FDC model when seeking consent from families. While the FDC Workshops promote the collaborative requesting model14, it was only used in 16 per cent of cases where consent was sought from families for donation in 2013. However, OTA advised the ANAO that it did not expect the FDC Workshop participants to apply the collaborative requesting model as it had not yet been selected as the national model, and OTA is currently conducting a trial of the collaborative approach and another model, the designated requestor model, in select hospitals.15 The results of the trial, which is expected to be finalised in June 2015, will help OTA select the model to be adopted nationally. Confirming which model will be adopted nationally should improve the consistency of approach used to seek consent from families by enabling OTA to promote and monitor its application nationally through the DonateLife Network.
22. There would also be benefit in OTA continuing to monitor opportunities to improve the FDC Workshops in light of feedback from donor families, training participants and the state-based DonateLife Agencies. For example, national studies of donor family experiences have provided an indication of areas the FDC Workshops may need to address, such as the clarity of language used by medical staff. The introduction of internal performance indicators, such as the consistency of approaches towards donor families, would assist with assessing the effectiveness and reach of the Package, as no indicators are currently in place.
Community Awareness and Education (Chapter 3)
23. OTA introduced a National Community Awareness and Education Program, as required under Measure 5 of the national reform program. The Program: included a National Communications Framework and Charter aimed at establishing a nationally consistent and coordinated approach to community awareness and education; and aims to provide stakeholders with access to information and resources.
24. There has been a high take-up of key elements of the Charter among the 13 community organisations which were signatories to the Charter. While OTA provides a range of forums for stakeholders to collaborate and share information, the effectiveness of its key forum, the Charter Signatories Committee, appears to have diminished over time. Well established forums, such as the Charter Signatories Committee, can provide a valuable opportunity for ongoing consultation and collaboration with stakeholders, and OTA could usefully reflect on how best to harness this potential going forward.
25. The largest financial component of the Program was an advertising campaign conducted by OTA from 2010 to 2012, at a cost of $13.8 million. OTA adopted an evidence-based approach to selecting a campaign message, which focussed on promoting family discussion about organ and tissue donation. To assess the effectiveness of the advertising campaign, OTA commissioned tracking research to monitor outcomes against key campaign benchmarks.16
26. The tracking research for Phase 1 of the campaign indicated that while there had been an overall increase in family discussion levels, males and people aged 18 to 29 years old and over 65 years old were less likely to have discussed their donation wishes. The final wave of research for Phase 2 of the campaign indicated that there was still potential to improve the knowledge and awareness of people aged 18 to 29 years old as they were the most likely to be influenced by the campaign but also the least likely to have seen the advertising. In summary, the tracking research indicated that Phase 1 of the campaign (at a cost of $9.2 million) achieved improved outcomes against the campaign benchmarks, while Phase 2 (at a cost of $4.6 million) delivered a more marginal return on investment, serving largely to help maintain the outcomes of Phase 1.
27. Consistent with the Guidelines on Information and Advertising Campaigns by Australian Government Departments and Agencies (March 2010), OTA: tested the advertising materials with focus groups; submitted the relevant information to the Independent Communications Committee; and completed internal evaluations of each phase of the campaign.
28. OTA has conducted eight Community Awareness Grants Rounds, which are promoted as competitive rounds for the provision of Australian Government financial assistance. The transparency of OTA’s grants administration can be improved by more clearly outlining the grants assessment process in the guidelines for applicants. For example, OTA advised the ANAO that it reconsiders applications which have equal scores in light of points of difference and this can result in a further assessment of value for money. Further, scope, reach and impact are all components of assessing value for money, but this is not reflected in OTA’s grants guidelines. OTA also provides funding to organisations through an unsolicited application process, which is not documented on OTA’s website or in the grant guidelines. The ANAO identified one applicant that was unsuccessful in a competitive grant round but subsequently received funding for the same activity as an unsolicited application. To improve equity and transparency, OTA should review its grants administration with a focus on informing potential grant funding applicants of all sources of available funding and the assessment process applying to these sources.
29. OTA is responsible for leading and coordinating an annual national awareness week, known as DonateLife Week. OTA advised the ANAO that the focus for the week is primarily a media and public relations campaign which is supported by sector-driven activities as a secondary focus. OTA commissioned media analysis of the 2014 DonateLife Week which indicated that events during the week can be very effective at generating media attention. At present, DonateLife Week events occur in limited locations and there is scope for OTA to encourage a broader geographic reach and range of events, which may assist in generating additional media interest during DonateLife Weeks. In particular, there would be benefit from OTA encouraging greater participation in DonateLife Week by non-government stakeholders. Introducing broad targets for the level of activity undertaken by corporate and community supporters, in the same manner as it does for social media, may assist OTA to focus efforts on increasing the number and reach of activities hosted by supporters.
30. OTA has developed a range of educational resources, including specific resources targeted at CALD communities, which have been identified by research commissioned by OTA as a priority group. OTA undertook extensive consultation with faith and cultural leaders to develop a collection of published statements of support for organ and tissue donation, as well as translated videos and brochures. Planning is underway to produce a second wave of resources aimed at addressing identified misconceptions about organ and tissue donation that are specific to faith and cultural communities.
31. OTA identified in its National Communication Strategy 2013–14 four performance indicators to measure the effectiveness of the National Community Awareness and Education Program. For 2013, in relation to the four performance indicators, OTA:
- met the target for: Australians have had a family discussion about organ and tissue donation (achieved 75 per cent against a 70 per cent target);
- did not meet the targets for the two indicators of: Australians knowing their family members’ wishes (achieved 53 per cent against a 68 per cent target); and Australians understanding that family consent is required for donation to proceed (achieved 70 per cent against a 74 per cent target)17; and
- achieved a 1.3 per cent increase in the number of registrations on the AODR.18
Support for Donor Families (Chapter 4)
32. Under Measure 6 of the national reform program, OTA introduced the National Donor Family Support Service (NDFSS) in 2011 to provide a tailored and nationally consistent program of support for donor families.
33. To implement the NDFSS, OTA provides funding to the states for Donor Family Support Coordinators (DFSCs). OTA revised a range of information resources for families and developed guidelines for DFSCs and Donation Specialist Coordinators on how to provide donor family support post-donation. At present, the guidelines do not outline the type of support to be provided to families in the hospital setting and should be enhanced to provide this guidance. Further, while the guidelines outline the type of support families should be provided post-donation, a national study of donor family experiences during 2010 and 2011 and released in 2014, indicated that there were varying levels of support being provided to donor families. For example, while DonateLife Agencies are required to contact donor families within 24 to 36 hours of donation, 22 per cent of family members did not receive a phone call following donation.19
34. To assess the effectiveness of support for donor families, OTA had two performance indicators in place which were discontinued in 2012–13.20 OTA reported in its annual report that it had met these indicators. However, ANAO analysis indicated that the basis for measuring achievement against the first performance indicator was too narrow to support an assessment that the indicator had been met. Further, OTA had collected insufficient information from DonateLife Agencies to inform an assessment of achievement against the second indicator. There have been no new indicators introduced to date, and consequently, OTA is not in a position to assess the implementation of Measure 6, relating to support for donor families. As a starting point, OTA should develop internal performance indicators to help assess the effectiveness of donor family support services.
Measurement and reporting (Chapter 5)
35. Consistent with the national reform program, OTA introduced a national data collection tool, known as the DonateLife Audit21, to assess state and national potential for organ donation rates, identify missed donation opportunities and determine the overall consent rate for organ donation. This information complements the Australia and New Zealand Organ Donation (ANZOD) Registry by providing data about hospital deaths in the context of organ donation.
36. The DonateLife Audit is limited to the DonateLife Network and does not collect information about eye and tissue donation.22 Further, while the DonateLife Audit reports information on organ donation after brain death (DBD), it does not report information about donation after circulatory death (DCD). This limits OTA’s capacity to report on the total number of potential donors, the donor family request rate and the consent rate. OTA is planning to develop a definition of the circumstances that will determine a potential DCD donor, which no country has yet developed, to improve consistency in capturing information about potential DCD donors. OTA’s planned enhancements will further improve the usefulness of the information collected through the DonateLife Audit.
37. OTA’s annual reports indicate that performance against indicators such as deceased donors per million population (dpmp) and number of donors has improved since the commencement of the national reform program, but decreased slightly in 2014.23 However, OTA is not achieving the targets set for the program’s quantitative performance indicators: donor family request rate and donor family consent rate.24 OTA advised the Senate Community Affairs Legislation Committee in February 2015 that the decline was partly attributable to the variability of donation outcomes between states and territories. OTA also highlighted a lack of consistency between states and territories in applying the Family Donation Conversation training, which OTA considered had adversely affected the family consent rate.
38. Since 2010, OTA has published on its website six-monthly performance reports on the implementation of the national reform program. The performance reports include information on the number of organ and tissue donors, number of transplant recipients and number of organs transplanted. OTA advised the ANAO that, in the future, these reports will only be prepared on an annual basis and the need for periodic reports will be assessed taking into account agency resources and priorities. The reports prepared to date do not include information about the number of registrations on the AODR. To provide a holistic view of the impact of the national reform program, there would be merit in OTA including the number of registrations in its performance reports.
Summary of entity response
39. The proposed audit report was provided to the Australian Organ and Tissue Donation and Transplantation Authority (OTA). OTA’s summary response to the proposed report is provided below, while the full response is provided at Appendix 1.
The aim of the Australian Government’s national reform programme is to implement a nationally coordinated world’s best practice approach to organ and tissue donation for transplantation in collaboration with the states and territories, clinicians and the community sector. Organ donation is a rare event, only around 1-2% of people who die in hospitals, die in the specific circumstances required to be a potential organ donor.
The Organ and Tissue Authority (OTA) thanks the generous Australians and their families who save and transform the lives of transplant recipients through organ and tissue donation.
The OTA notes the audit report’s conclusions and agrees with the recommendations of the proposed report.
Recommendations
|
Recommendation No.1 Para 3.13 |
To better harness the capacity of the organ and tissue donation sector and extend the reach of community awareness and education activities, the ANAO recommends that OTA more actively facilitate collaboration between Charter signatories through established forums. OTA response: Agreed. |
|
Recommendation No.2 Para 3.52 |
To improve transparency and equity, the ANAO recommends that OTA review its grants administration, with a particular focus on informing potential applicants of all available sources of grant funding and the assessment process applying to each source. OTA response: Agreed. |
|
Recommendation No.3 Para 4.26 |
To improve the services provided to donor families, including those families for which consent is provided but donation does not proceed, the ANAO recommends that OTA:
OTA response: Part (a): Agreed. Part (b): Agreed, subject to consultation with state and territory governments. |
1. Introduction
This chapter provides an overview of the Australian Government’s national reform program to increase the rate of organ and tissue donation. It also provides an outline of the audit objective, criteria and approach.
Background
1.1 Australia’s rate of organ and tissue donation does not meet the current demand for transplantation. In 2014, an average of 1632 people were on organ transplant waiting lists each month, and in total, 1117 people received organ transplants. In the same year, 5553 people received tissue transplants.
1.2 To increase Australia’s national performance in organ and tissue donation, the then Australian Government established the National Clinical Taskforce on Organ and Tissue Donation (the Taskforce) in October 2006. The Taskforce was asked to provide evidence-based advice on ways to increase the rate of organ and tissue donation with a view to informing the prospective reform agenda.25 The final report, submitted by the Taskforce to the Government in January 2008, identified systemic problems with the Australian organ donation and transplantation sector and made 51 recommendations to improve the performance of Australia’s donation and transplantation system.
National reform program
1.3 On 2 July 2008, the Australian Government announced a national reform program to ‘establish Australia as a world leader in organ donation for transplantation’.26 Endorsed by the Council of Australian Governments (COAG), the national reform program committed $136.4 million in new Australian Government funding over four years (2008–2012) to improve access to transplants through a nationally coordinated approach to organ and tissue donation.
1.4 The national reform program had two objectives: to increase the capability and capacity within the health system to maximise donation rates; and raise community awareness and stakeholder engagement across Australia to promote organ and tissue donation. Nine measures were endorsed by COAG aimed at achieving the two broad program objectives:
- Measure 1: A new national approach and system – a national authority27 and network of organ procurement organisations.
- Measure 2: Specialist hospital staff and systems dedicated to organ donation.
- Measure 3: New funding for hospitals.
- Measure 4: National professional awareness and education.
- Measure 5: Coordinated ongoing community awareness and education.
- Measure 6: Support for donor families.
- Measure 7: Safe, equitable and transparent national transplantation process.
- Measure 8: National eye and tissue donation and transplantation.
- Measure 9: Additional national initiatives, including living donation programs.
1.5 This audit focussed on Measures 4 to 6 highlighted above, relating to: professional education; community awareness; and support for donor families.
Professional awareness and education (Measure 4)
1.6 Measure 4 of the national reform program is intended to facilitate ongoing development and training for clinical and professional staff involved in organ and tissue donation. The measure is expected to drive cultural and organisational change in public and private hospitals and contribute to the front-end clinical work of increasing donation and transplantation rates.
Community awareness and education (Measure 5)
1.7 Measure 5 aims to increase public knowledge about organ and tissue donation and build confidence in Australia’s donation system. The provision of nationally consistent information about organ and tissue donation is expected to contribute to an increase the number of families consenting to donation.
Support for donor families (Measure 6)
1.8 Measure 6 provides for a nationally coordinated approach to support the families of deceased donors. New funding was provided for the development of a national donor family support program so that donor families receive the support they need in the hospital setting and afterwards.
Organ donation in Australia
1.9 The Australian organ and tissue donation system is based on an ‘informed consent’ (or opt-in) model, whereby individuals agree to donate their organs and tissue in the event of their death.28 The Australian Organ Donor Register (AODR), administered by the Department of Human Services, enables individuals to record their consent or objection to becoming an organ and/or tissue donor. As at 31 January 2015, there were approximately six million registrations on the AODR.29
1.10 Regardless of whether an individual has provided consent for donation, the practice in Australia is to also seek agreement from a donor’s next of kin before donation proceeds.30 The Australian Organ and Tissue Donation and Transplantation Authority (OTA) reported in its 2014 performance report that in 2014, there were approximately 700 potential donors and 680 requests were made to their next of kin for organ and tissue donation to proceed. Of these requests, consent was given in 61 per cent of cases. This resulted in the transplantation of 1193 organs, as a number of organs can be donated by each donor.
1.11 The number of deceased donors per million population (dpmp) is the most common measure used for international comparisons of performance in organ and tissue donation. In the decade prior to the launch of the national reform program in 2008–09, Australia’s donor rate remained relatively constant at around 10 dpmp. This figure rose to 16.9 dpmp in 2013 and then decreased slightly to 16.1 in 2014.31
The Australian Organ and Tissue Donation and Transplantation Authority
1.12 OTA was established in January 2009 as the first measure of the national reform program. OTA was intended to lead a coordinated national approach to organ and tissue donation in partnership with the states and territories (states), clinicians and the community sector. Operating under the Australian Organ and Tissue Donation and Transplantation Authority Act 2008, OTA is an independent statutory authority within the Department of Health portfolio.32
1.13 At 30 June 2014, OTA employed 26.2 full-time equivalent staff, including a Chief Executive Officer and one Senior Executive Service officer. A three-tier committee structure is in place to provide program governance and sector-specific advice. OTA reports publicly on the implementation of the national reform program, as well as broader measures associated with organ and tissue donation, in performance reports33 and through its annual report.
1.14 The Australian Government announced on 13 May 2014 that OTA would merge with the National Blood Authority by 1 July 2015.
DonateLife Network
1.15 OTA has overall national responsibility for the implementation of the nine COAG reform measures, working in collaboration with state and territory based DonateLife34 Agencies. Under Measure 1 of the national reform program, DonateLife Agencies were established in each state to manage the donation process at the state level. Led by their respective State Medical Directors and a National Medical Director, DonateLife Agencies are responsible for the coordination of organ and tissue donations, professional and clinical education, support for donor families, community awareness and data collection.
1.16 OTA provides Australian Government funding to each state government to employ DonateLife staff in 72 hospitals35 and the DonateLife Agencies. At the end of June 2014, the DonateLife Network included 175 hospital-based medical and nursing specialists in organ and tissue donation and 100 staff (principally specialist nurses) in the eight DonateLife Agencies. The National Roles and Responsibility Guidelines36, developed by OTA in consultation with the state governments, inform the recruitment of DonateLife staff.
1.17 Funding to the states is provided through two-year funding agreements which require each jurisdiction to maintain an organ and tissue donation service delivery model consistent with the national reform approach and in accordance with relevant ethical guidelines and clinical protocols.37 Funding agreements include an agreed performance and reporting framework to enable OTA to monitor progress in each jurisdiction.
Organ and Tissue Donation Reform Package: Mid-Point Implementation Review
1.18 In 2011, the then Parliamentary Secretary for Health and Ageing commissioned a review of the implementation of the national reform program—the Organ and Tissue Donation Reform Package: Mid-Point Implementation Review Report. Overall, the review found that while significant progress had been achieved for some measures, only moderate or relatively little progress had been made in implementing the remaining measures.38 The report observed that OTA had made significant progress in establishing the DonateLife Network and supporting the placement of dedicated clinical staff in hospitals.
1.19 The report identified a number of areas for improvement, including: strengthening clinical practice improvement programs and establishing a clinical governance framework; enhancing national performance measurement; and expanding professional education for the DonateLife Network and broader hospital staff. A focus on these areas is reflected in OTA’s strategic priorities going forward, as agreed between the Australian and state governments.
Audit objective, criteria and scope
1.20 The audit objective was to assess the effectiveness of OTA’s administration of community awareness, professional education and donor family support activities intended to increase organ and tissue donation.
1.21 To assist in evaluating OTA’s performance in terms of the audit objective, the ANAO developed the following high-level criteria relating to the administration of community awareness, professional education and donor family support activities:
- OTA plans and designs targeted activities;
- OTA effectively administers activities in accordance with relevant frameworks39; and
- OTA assesses and reports on the effectiveness of activities.
1.22 The audit scope included an assessment of OTA’s performance in relation to Measures 4, 5 and 6 of the national reform program.40 For Measure 4, the audit focussed on OTA’s Professional Education Package. The audit did not assess: the other six reform measures; the Department of Human Services’ administration of the AODR; or the legislation and policy regulating organ and tissue donation in Australia.
Audit methodology
1.23 The ANAO’s audit methodology included:
- interviewing:
- relevant OTA staff, including State Medical Directors and a number of DonateLife Agency staff; and
- stakeholders, including non-government organisations; and
- reviewing:
- advertising, awareness raising and professional education materials and associated evaluation results;
- compliance with the Australian Government’s 2010 Guidelines on Information and Advertising Campaigns by Australian Government Departments and Agencies;
- compliance with the July 2009 and July 2013 Commonwealth Grant Guidelines; and
- relevant performance measurement and reporting material.
1.24 The audit was conducted in accordance with the ANAO Auditing Standards at a cost to the ANAO of approximately $393 588.
Structure of report
1.25 The structure of the audit report is outlined in Table 1.1.
Table 1.1: Structure of chapters
|
Chapter |
Overview |
|
2. Professional Education |
Examines OTA’s Professional Education Package, including the development of the Family Donation Conversation Workshops. |
|
3. Community Awareness and Education |
Examines the management and effectiveness of OTA’s Community Awareness and Education Program. |
|
4. Support for Donor Families |
Examines the donor family support resources and services funded by OTA. |
|
5. Measurement and Reporting |
Examines OTA’s internal and external reporting, including its key performance indicators. |
2. Professional Education
This chapter examines OTA’s Professional Education Package, including the development of the Family Donation Conversation Workshops.
Introduction
2.1 Under Measure 4 of the national reform program, OTA is required to coordinate an ongoing, nationally consistent and targeted program of professional development and training for clinicians and care workers involved in organ and tissue donation. The program, which includes OTA’s Professional Education Package (the Package), is expected to build on existing programs, including the Australasian Donor Awareness Program (refer to paragraphs 2.3 to 2.8).
2.2 OTA introduced the Package in 2012.41 Initially the Package included two Australasian Donor Awareness Program workshops and two Family Donation Conversation (FDC) Workshops—one core and one practical.42 OTA was revising the Package during this audit, to include: an Introductory Donation Awareness Training workshop; the two FDC Workshops; and advanced training to focus on current issues.43
Australasian Donor Awareness Program
2.3 The Australasian Donor Awareness Program has been delivered in Australia since 1994 and is intended to provide participants with a greater understanding of organ and tissue donation and the skills to sensitively conduct conversations with families about organ and tissue donation. The workshops are aimed at staff involved in end-of-life care, including intensivists.44 The program was managed by the Australian Red Cross Service until OTA assumed responsibility on 30 June 2010.
2.4 As part of the Australasian Donor Awareness Program, OTA delivered an ongoing training schedule comprising two workshops:
- general workshops: designed for registered nurses from critical care, emergency and operating theatres, allied health and palliative care professionals, social workers, chaplains and pastoral care workers; and
- medical workshops: designed for intensivists and trainees in intensive and emergency medicine, and intended to provide an overview of the organ and tissue donation process and information on communicating with and caring for families.
2.5 The program was revised following a review of the Professional Education Package by OTA in 2013, which identified some duplication with the training provided by the College of Intensive Care Medicine (CICM). From July 2014, the medical workshop was discontinued and its key grief and bereavement components were included in the core FDC Workshop, discussed in the next section.
2.6 The remaining general workshop will be replaced with an Introductory Donation Awareness Training workshop, which is currently being developed. The introductory workshop will provide a general overview of organ and tissue donation to DonateLife Network staff, hospital-based staff and students. OTA advised the ANAO that it has rescheduled the introduction of the introductory workshop from July 2014 to May 2015.
2.7 In its annual report, OTA does not report on the number of participants who have attended the Australasian Donor Awareness Program training. However, in its March 2014 report to the Australian Health Ministers’ Advisory Council, OTA reported that 67 workshops had been held with over 1000 participants since the introduction of the Professional Education Package in 2012.45
2.8 OTA does not have internal performance indicators to assess the effectiveness of the Australasian Donor Awareness Program. There would be benefit in OTA introducing internal performance indicators for the Introductory Donation Awareness Training workshop, following its launch, to measure and assess its effectiveness and reach.
Family Donation Conversation Workshops
2.9 The FDC Workshops were introduced in 2012 as part of OTA’s Professional Education Package. They are directed to health professionals and are a means for promoting a nationally consistent and best practice approach to requesting consent for donation from potential donors’ next of kin, and to assist families to make a decision in relation to organ and tissue donation. The introduction of the workshops was considered necessary as practices varied between states and in some instances between hospitals in the same state.
Development of the workshops
2.10 OTA engaged an Australian training provider in April 2011 to develop family donation conversation training: one concise module to be integrated into the Australasian Donor Awareness Program; and a comprehensive one-day workshop.46 The purpose of the workshops was to provide participants with the skills to inform families about donation and support them to make a donation decision.
2.11 A pilot of the one-day workshop developed by the Australian provider was held in October 2011. Participant feedback on the pilot indicated that it did not adequately reflect a clinical environment and therefore, did not meet OTA’s requirements. Consequently, the training materials were provided to a group of DonateLife clinical subject experts in 2011 to finalise. The materials comprise the basis for the current practical FDC Workshop (refer to paragraph 2.2).
2.12 In June 2011, OTA also engaged a United States training provider, the Gift Of Life Institute (the Institute), to deliver two of its training workshops in Australia.47 OTA understood that the Institute was the only known organisation with a request for consent training module and advised the ANAO that the Institute’s workshops were expected to provide an advanced level of training for clinicians, whereas the training being developed by the Australian provider was expected to provide practical training on communicating sensitively.
2.13 The Institute delivered two of its workshops under its first contract.48 Based on this material, the Institute was engaged under a second contract to develop and deliver a revised workshop, as well as train DonateLife Network staff to deliver the workshop.49
Delivery of the workshops
2.14 The FDC Workshops commenced in March 2012—one year after the planned delivery date. Since the core FDC Workshops were introduced across all states in 2012, OTA has reported that:
- 30 core FDC Workshops have been held, with more than 700 participants; and
- 35 practical FDC Workshops have been delivered to 401 participants.
2.15 The Institute prepared two reports based on the training it delivered across six states during March and May 2012. The reports identified some areas for improvement in the training, which the Institute implemented.50
2.16 The FDC Workshops promote a consistent model for requesting consent for donation from families, known as the collaborative requesting model.51 The reports concluded that in some workshops, there was a lack of acceptance from participants about the need to change the family consent request approach. There were also concerns raised by participants regarding the proposed change in their roles and that the collaborative requesting model was potentially coercive. Overall, the second report noted that the participants did not have a clear understanding of the initiatives being progressed by OTA, including the change in consent request approach.
2.17 OTA and the Institute revised the FDC materials between September 2013 and August 2014, to incorporate the family communication elements from the discontinued medical Australasian Donor Awareness Program workshop.52 The revised FDC Workshop was delivered as a pilot in March 2014. The Institute prepared a further report about the pilot and did not recommend any further changes to the training.
2.18 The revised workshop was also delivered to the CICM and the Australian and New Zealand Intensive Care Society in April 2014.53 Feedback from these bodies was that the training was an improvement on the previous iteration but that it could be further enhanced. Specific feedback regarding the wording and relevance of some materials was provided to OTA and this feedback was actioned, where OTA considered it appropriate.
2.19 There would be benefit in OTA continuing to monitor opportunities to improve the FDC Workshops. National studies of donor family experiences provide an indication of issues which the FDC Workshops may need to address further. For example, a national study of donor family experiences during 2010 and 2011 suggested that the language used by medical staff in discussion with families was an issue in some instances.54 Eighteen per cent of study participants only ‘somewhat’ agreed that the language used by medical staff was clear and easy to understand and 14 per cent of participants only ‘somewhat’ agreed that they had sufficient opportunity to ask questions.
2.20 There is also scope for OTA to consider introducing variations of the FDC Workshops to more effectively target the needs of staff involved in end-of-life patient care. In discussing the review of the Professional Education Package implemented in 2014, members of OTA’s Jurisdictional Advisory Group55 suggested that an abridged version of the FDC could be introduced for staff who are not involved in requesting consent but who are involved with supporting donor families.
Measurement of the workshops
2.21 OTA collects feedback from participants following the FDC Workshops. OTA advised the ANAO that feedback is reviewed by facilitators at the conclusion of the first day of training so that any issues or concerns are addressed on the second day. Further, OTA’s National Training Coordinator reviews feedback from each workshop and discusses any issues with facilitators and local DonateLife Agencies, if necessary. The Coordinator also provides feedback to OTA to be considered for review and so that feedback can be circulated to all facilitators.
2.22 As mentioned in paragraph 2.14, OTA reports on the number of FDC Workshop participants. However, OTA has not developed internal performance indicators for the FDC Workshops, to help assess their contribution to the professional training effort. Overall, the intended outcome of the Professional Education Package is to contribute to an increase in the family consent rate. There is scope for OTA to consider the applicability of internal performance indicators, such as the consistency of approaches towards donor families (refer to paragraphs 2.23 to 2.25).
Effectiveness of the workshops
2.23 Overall, the FDC Workshops are targeted at improving the family consent rate. In 2014, for the first year since the commencement of the national reform program, there was a decline in the number of deceased organ donors, which OTA has partly attributed to lower family consent rates in some states. OTA advised the Senate Community Affairs Legislation Committee in February 2015 that there was a clear difference in family consent outcomes when a trained requester discussed organ donation with families and when an intensivist discussed donation with families. To address variability in family consent rates, OTA acknowledged that it needed to reinforce its expectation that relevant staff undertake the FDC training and apply the training when seeking consent from families.
2.24 The FDC Workshops were introduced to promote a nationally consistent and best practice approach to requesting consent from families. As discussed in paragraph 2.16, the FDC Workshops promote the collaborative requesting model. The 2013 DonateLife Audit56 reported that in 61 per cent of cases where consent was sought from families for donation, the request was made by the treating intensivist, and a collaborative requesting model was used in only 16 per cent of cases.
2.25 However, OTA advised the ANAO that it did not expect the FDC Workshop participants to apply the collaborative requesting model as it had not yet been selected as the national model. OTA is currently conducting a trial of the collaborative approach and another model, the designated requestor model, in select hospitals.57 Based on the results of the trial, which is expected to be finalised in June 2015, and following consultation within the DonateLife Network and state governments, OTA will select the model to be adopted nationally. Confirming which model to adopt nationally will assist to improve the consistency of approaches to requesting consent from families as it will enable OTA to promote and monitor the application of the selected model within the DonateLife Network.
Conclusion
2.26 As required under Measure 4 of the national reform program, OTA introduced the Professional Education Package to address an identified gap in education. The Package incorporates the existing Australasian Donor Awareness Program, which is expected to be replaced by the Introductory Donation Awareness Training workshop in May 2015.
2.27 The Package also incorporates the core and practical FDC Workshops, which over 1100 participants have attended since they were introduced in 2012. However, there were some shortcomings with the development and delivery of the FDC Workshops; in particular, the engagement of a provider which did not fully meet OTA’s training requirements, and delays in the introduction of the Workshops.
2.28 In 2014, the number of deceased organ donors decreased slightly, which OTA has partly attributed to low family consent rates in some states. OTA acknowledged that it needed to reinforce its expectation that relevant staff undertake and apply the FDC training when seeking consent from families. Confirming which model to adopt nationally will enable OTA to promote and monitor the application of the selected model within the DonateLife Network and assist with improving the consistency of approaches to donor families.
2.29 Further, there would be merit in OTA continuing to assess the need for enhancements to the FDC Workshops, as well as to the Professional Education Package as a whole. There are no internal performance indicators relating to the Australasian Donor Awareness Program or FDC Workshops to help OTA assess their contribution to professional training. The introduction of internal performance indicators would assist with assessing the effectiveness and reach of the Professional Education Package.
3. Community Awareness and Education
This chapter examines the management and effectiveness of OTA’s Community Awareness and Education Program.
Introduction
3.1 To improve public knowledge about organ and tissue donation, Measure 5 of the COAG national reform program provided for coordinated and ongoing community awareness and education.58 The three key elements of Measure 5 are: a national community awareness framework; a national community awareness charter; and an ongoing national community awareness and education program.
3.2 OTA’s National Communication Framework and Charter form part of the National Community Awareness and Education Program, which has included a national advertising campaign running from 2010 to 2012. Other elements of the program are: a grants program; a national awareness week; information and education resources; community outreach; and media and public relations.
National Community Awareness and Education Program
3.3 The overall aim of OTA’s Community Awareness and Education Program is to contribute to increases in organ and tissue donation. OTA promotes a ‘Discover, Decide and Discuss’ message directed to the community:
- Discover: promote nationally consistent factual information about organ and tissue donation, the benefits of transplantation and the importance of family discussion and knowledge of each other’s donation decisions.
- Decide: encourage Australians to make an informed decision about becoming a potential donor and register their decision on the Australian Organ Donor Register (AODR).
- Discuss: increase the number of Australian families that discuss and know each other’s decisions on organ and tissue donation.
OTA’s communications framework
3.4 A National Communications Framework (the Framework) was developed by OTA in early 2009 in consultation with sector stakeholders to: establish the parameters of a nationally consistent and coordinated approach to community awareness and education; and provide stakeholders with access to useful information and resources.
3.5 In November 2009, OTA launched the DonateLife brand and website as part of a national communications platform for the organ and tissue sector. The DonateLife logo became the official symbol for organ and tissue donation in Australia, featuring in all materials developed by OTA. Stakeholders were also encouraged to use the DonateLife logo alongside their existing brand. The state organ and tissue donation agencies became the DonateLife Agencies and adopted the DonateLife name and brand. In establishing a social media presence, OTA created a DonateLife Facebook, Twitter, Instagram and Twibbon identity to assist with community awareness and education.
3.6 OTA also introduced the National Communications Charter (the Charter), to encourage governments and stakeholders to sign up to best practice principles for community awareness, education and communication activities, including a commitment to use consistent language and messages. There has been a high take-up of key elements of the Charter among the 13 community organisations which were signatories to the Charter. For example, 90 per cent of the community organisation signatories use the national logo in their communications, in conjunction with their own branding.
3.7 In 2014, OTA developed a new DonateLife Stakeholder Engagement Framework to replace the National Communications Framework and Charter. The new framework incorporates three stakeholder tiers:
- DonateLife Partners are those who have organ and tissue donation for transplantation as part of their core business, including current Charter signatories;
- DonateLife Community Partners represent a range of sporting clubs, schools, small businesses and foundations who want to be associated with DonateLife but do not have organ and tissue donation or transplantation as their core business; and
- DonateLife Corporate Partners from the business sector seeking to promote and facilitate education and awareness of organ and tissue donation with their employee and customer base.
3.8 As at January 2015, OTA had 52 DonateLife Partners, 20 DonateLife Community Partners and five Corporate Partnerships. Each partner has signed a DonateLife Partnership Agreement, committing to the promotion and distribution of the DonateLife key messages and materials and use of the partner logo, in addition to organising a minimum of one community awareness activity per year.
3.9 The previous Framework outlined the responsibilities of the Australian Government and Charter signatories in relation to community awareness and education. The ANAO assessed the extent to which OTA has fulfilled its responsibilities under the Framework, with the results summarised in Table 3.1.
Table 3.1: List of OTA’s responsibilities under the National Communications Framework
|
Responsibilities |
Status |
|
Provide communication materials and resources |
F |
|
Encourage the use of the national logo for organ and tissue donation |
F |
|
Make available publication quality logo kits |
F |
|
Maintain a dedicated website |
F |
|
Advise organisations where necessary on how to amend current activities to cater for the introduction of a new communications framework |
F |
|
Assist signatories in handling issues as they arise |
F |
|
Encourage and facilitate collaboration between signatories |
P |
|
Provide the opportunity to apply for funding for community awareness and education activities |
F |
Source: ANAO analysis and DonateLife National Communications Framework 2011.
Legend: F = fully met the responsibility.
P = partially met the responsibility.
3.10 Table 3.1 indicates that OTA has largely met its responsibilities under the Framework. However, there remains scope to more actively encourage and facilitate collaboration among Charter signatories. This is consistent with OTA’s obligations under the national reform program to develop a framework that encourages ‘stakeholders to collaborate and build on each other’s efforts and avoid unnecessary duplication of work, research and resources’.59
3.11 OTA advised the ANAO that it encourages collaboration and information sharing among Charter signatories through a range of mediums including committees, newsletters and emails. A key vehicle for collaboration is the Charter Signatories Committee, which is used for: OTA to update members on the progress of the national reform program, including the National Community Awareness and Education Program; and for Charter signatories to share their plans, demonstrate how they align with the national reform program and identify opportunities for sector participation. Information on events being planned by stakeholders is also shared at Charter Signatories Committee meetings and is included on a national calendar of events.60
3.12 While the Charter Signatories Committee was originally intended as a collaborative forum, its effectiveness in this respect appears to have diminished over time. The frequency of meetings has reduced from six-monthly to annually, and representatives from DonateLife Agencies have ceased attending meetings. Further, the minutes of meetings examined by the ANAO indicate that meetings now largely focus on the provision of information from OTA, with a lesser focus on identifying opportunities for collaboration. Established forums such as the Charter Signatories Committee provide a valuable opportunity for ongoing consultation and collaboration between OTA and stakeholders, and there would be merit in OTA reflecting on how best to harness this potential going forward.
Recommendation No.1
3.13 To better harness the capacity of the organ and tissue donation sector and extend the reach of community awareness and education activities, the ANAO recommends that OTA more actively facilitate collaboration between Charter signatories through established forums.
OTA’s response
3.14 Agreed.
Advertising campaign
3.15 Research undertaken in 200761 indicated that while over 90 per cent of Australians support organ and tissue donation, this level of support was not demonstrated in the proportion of actual donors. A number of factors can influence behaviour and attitudes in relation to organ and tissue donation, such as knowledge and beliefs about donation. This research and other research undertaken by two research agencies in 2009, informed OTA’s decision to focus its advertising effort on promoting family discussion about organ and tissue donation.
Campaign messaging and selection
3.16 OTA’s advertising campaign, ‘Discuss it today, OK’, was aimed at increasing awareness about the importance of family discussion among Australians. The campaign’s call to action, and the primary objective of the campaign, was for Australians to know, understand and accept the wishes of their family members by discussing organ and tissue donation and sharing their wishes with family members.
3.17 The primary target audience for the campaign was families as they are required to provide consent for organ donation to proceed. Three segments were identified within this primary target audience: people who were undecided about organ donation; people who had registered to be organ donors; and
non-registered donors who had decided to be organ donors.
3.18 To develop the campaign, OTA undertook a select tender process and approached five advertising agencies to provide submissions on a campaign which included: a television commercial, radio and print advertisements and internet banners.62 The campaigns proposed by the five agencies were tested by a research agency.63
3.19 The report issued by the research agency, summarising the results of the testing, advised that three of the five proposed campaigns had potential. However, the report noted that one of the proposed campaigns was a clear preference, and was recommended because each media component of the campaign (i.e. television and radio) tested well and contributed to a cohesive campaign. Further, the preferred campaign had the largest proportion of participants identifying it as their first choice among the tested campaigns. The tender evaluation panel, however, ranked OTA’s chosen campaign, ‘Discuss it today, OK’, higher than the recommended campaign following a value for money assessment.64
Campaign strategy
3.20 The campaign was undertaken in two phases at a cost of $13.8 million (refer to Table 3.2). Both phases were extended, with Phase 1 extended twice. These extensions were designed to supplement the primary phases of the campaign and to raise awareness during the 2011 and 2012 DonateLife Weeks. OTA commissioned an agency to undertake tracking research during the campaign to monitor its effectiveness65, and also used the results of the tracking research to inform the later phases of the campaign.
Table 3.2: Summary of campaign advertising phases
|
Phase |
Message |
Media channels |
Timeframe |
Cost 1 |
|
Phase 1 |
‘Discuss it today, OK’ |
Television, radio, magazines, outdoor, online and cinema |
May to June 2010 |
$6.4 million |
|
Extended Phase 1 |
‘Discuss it today, OK’ |
Online advertising and social video |
November 2010 to December 2011 |
$2.8 million |
|
Second extension of Phase 1 |
‘Any day is a good day to talk about it’ |
Television, print and online component |
February to May 2011 |
|
|
Phase 2 |
‘Know their wishes’ |
Television, print, online and outside advertising |
May to August 2011 |
$2.9 million |
|
Extended Phase 2 |
‘Know their wishes’ |
Television and online advertising |
February to April 2012 |
$1.7 million |
Source: ANAO analysis.
Note 1: These costs included: developing the campaign materials; purchasing media placements; producing and distributing materials; and undertaking the tracking research.
3.21 Phase 1 was launched with a call to action for family members to discuss their donation wishes—in effect for people to tell family members their wishes. This message was consistent with research undertaken in 2007 which showed that most respondents were in favour of a communications campaign that emphasised telling those close to them of their own wishes in relation to donation, rather than asking about the other person’s wishes (59 per cent and 30 per cent respectively). The tracking research results showed that Phase 1 of the campaign was effective at increasing: family discussion rates; awareness of family members’ wishes; and awareness that family consent is required for donation against benchmark levels (refer to paragraphs 3.31 to 3.36).66
3.22 The message for Phase 2 was developed in response to the tracking research, which showed that a higher proportion of people indicated that they had advised their family members of their donation wishes than the proportion of people who indicated they knew their family members’ donation wishes. Phase 2 focussed on the less popular message—to ‘ask’ family members about their wishes—in order to encourage people who were uncomfortable with initiating a discussion about organ and tissue donation. Overall, while the tracking research indicated that the Phase 2 campaign resulted in higher rates of discussion and awareness of the role of family consent, these outcomes were only marginally higher than those achieved in Phase 1 (refer to Table 3.3).
3.23 The second extension of Phase 1 and the extension of Phase 2 coincided with the 2011 and 2012 DonateLife Weeks. The message, ‘Any day is a good day to talk about it’ and associated advertising materials were specifically developed for the 2011 DonateLife Week. This revised message was expected to generate a sense of urgency for having the discussion about organ and tissue donation, as well as give people permission to initiate the discussion.
Testing
3.24 In addition to the testing outlined in paragraphs 3.18 to 3.19, OTA commissioned testing of revised campaign materials, consistent with the Australian Government’s campaign advertising guidelines then in effect (the advertising guidelines).67 This testing was conducted by the research agency which had earlier advised OTA, and was intended to provide assurance that the advertising messages were clear and that the advertisements had an impact across different demographics.
3.25 The Phase 1 campaign materials were tested four times. In the second round of testing, similar areas for improvement were identified as in the first round of testing despite OTA having made changes to address these issues. Of most significance was the recommendation made after testing to improve the clarity of the message in the television commercial about the need to have a discussion with family members regarding organ and tissue donation.68 This was identified as an area for improvement in the first, second and fourth rounds of testing for the Phase 1 materials.69 OTA advised the ANAO that it considered the recommendations made as a result of testing and implemented those changes considered appropriate.
3.26 In respect to the Phase 2 materials, areas identified for improvement in testing had been addressed by the second round of Phase 2 testing. However, there was limited testing undertaken of the Phase 2 messaging—particularly in regional areas—to demonstrate that this would be an effective message.70 OTA advised the ANAO that the Phase 2 testing methodology was recommended by the research agency based on its available budget.
Review and approval by the Independent Communications Committee
3.27 Under the 2010 advertising guidelines, the role of the Independent Communications Committee (ICC)71 was to consider whether advertising campaigns valued at more than $250 000 complied with key aspects of the advertising guidelines, and provide advice to the relevant agency regarding compliance. In total, OTA met with the ICC eight times and submitted for consideration its advertising materials, Chief Executive certification72, compliance statement in relation to the advertising guidelines, testing results, and media plan.
3.28 The advertising guidelines also required that campaigns comply with relevant legislation and procurement rules.73 OTA reported a legislative breach to the ICC in its October 2009 ICC submission. OTA noted that there were breaches relating to the financial approval requirements established by the Financial Management and Accountability Regulations (1997) in relation to the appointment of public relations and research companies.74 OTA reported that it subsequently reviewed and improved internal business processes as a result of identifying these breaches.
Performance and outcome indicators for Phases 1 and 2
3.29 OTA identified a range of internal performance indicators for Phases 1 and 2 of the campaign:
- website statistics, online social media activity and online search engine key word hits;
- the number of enquiries from the general public to the DonateLife Network;
- news and editorial media coverage and post campaign analysis of media placements by the preferred Australian Government provider; and
- the number of new registrations on, or updates to, the AODR.
3.30 Phase 1 of the campaign also included a performance indicator relating to the number of families who initiate the discussion about donation in a hospital setting. OTA advised that this performance indicator was not used in Phase 2 as it would be difficult to directly attribute such an outcome to the advertising campaign.
3.31 OTA’s key internal outcome indicators for tracking the effectiveness of the campaign were the levels of:
- family discussion in the past 12 months;
- reporting the discussion as memorable;
- awareness of family members’ wishes; and
- knowledge of the role of family consent.
3.32 As discussed in paragraph 3.20, OTA engaged an external agency to undertake a benchmark survey and six waves of tracking research throughout the campaign.75 Table 3.3 summarises the results of the tracking research for OTA’s key outcome indicators.
Table 3.3: Tracking of OTA’s key outcome indicators
|
Indicator |
Benchmark (%) |
Wave 1 (%) |
Wave 2 (%) |
Wave 3 (%) |
Wave 4 (%) |
Wave 5 (%) |
Wave 6 (%) |
|
|
|
Phase 1 |
Phase 2 |
||||
|
Had a family discussion (in the past 12 months) |
48 |
59 |
58 |
53 |
57 |
60 |
58 |
|
Discussion was memorable |
n/a |
n/a |
83 |
81 |
82 |
81 |
81 |
|
Awareness of family members’ wishes |
51 |
60 |
57 |
54 |
55 |
57 |
56 |
|
Awareness that consent is required |
64 |
72 |
73 |
70 |
71 |
74 |
70 |
Source: OTA internal document.
Note: The Wave 6 tracking research also asked whether families had ever had a discussion regarding organ and tissue donation and reported a 77 per cent response rate. OTA commissioned a seventh wave of research which was carried out in 2013, after the advertising campaign had ended. The response rate for whether families had ever had a discussion about organ and tissue donation was 75 per cent. The research results for Wave 7 are reported in Table 3.6.
3.33 The research indicated that overall, the outcomes for Phase 1 of the campaign tracked above the three benchmark indicators adopted for the campaign, while in Phase 2, overall outcomes improved marginally against two indicators and remained stable against one. In summary, Phase 1 of the campaign (at a cost of $9.2 million) achieved improved outcomes against the campaign benchmarks, while Phase 2 (at a cost of $4.6 million) delivered a more marginal return on investment, serving largely to help maintain the outcomes of Phase 1.
3.34 Overall, between the benchmark and Wave 6 results, there was a 10 per cent increase in family discussions; a five per cent increase in the awareness of family members’ wishes; and a six per cent increase in the proportion of people who understood that family consent is required for donation to proceed.
3.35 The tracking research for Phase 1 noted that while there had been an increase in family discussion levels, males and people aged 18 to 29 years old and over 65 years old were less likely to have discussed their donation wishes. Consequently, in its evaluation of Phase 1, OTA identified people aged 18 to 29 years old, males and people aged over 65 years old as groups which required further attention. OTA advised the ANAO that it implemented a range of campaign initiatives targeted at young adults, including media strategies, videos, postcards and a Youth Support Kit. Notwithstanding these initiatives, the Wave 6 research results indicated that there was still potential to improve the knowledge and awareness of people aged 18 to 29 years old as they were the most likely to be influenced by the advertising campaign but the least likely to have seen the advertising.
3.36 There was a six per cent increase in awareness that consent is required between the benchmark and Wave 6 testing (to 70 per cent). However, awareness among people aged 18 to 29 years old in Wave 6 was lower than the general benchmark level of 56 per cent. Although this is a low rate of awareness for young people, it represented an improvement of three per cent against the benchmark level (53 per cent).
Objectives of the campaign
3.37 The three overarching objectives of the campaign were to:
- encourage Australians to discuss organ and tissue donation with their families and to understand the role of the family in providing consent for donation to proceed;
- increase the number of Australian families who know, accept and commit to uphold each other’s wishes; and
- increase the number of families who consent to and initiate organ and tissue donation requests.
3.38 Through the tracking research results, OTA monitored: discussion levels; awareness that family consent is required for donation to proceed; and the proportion of families who indicated that they knew their family members’ wishes (refer Table 3.3). In Wave 6 of the tracking research, participants were also asked whether they would uphold their family members’ wishes regarding donation, however, this question was not included in the earlier waves of research. Ninety-two per cent of the respondents indicated they would uphold their family members’ wishes.
3.39 During the course of the campaign, there was no information available on the level of family initiated discussion in hospital settings about organ and tissue donation as this information was only collected from 2013 using the DonateLife Audit tool.
3.40 Contributing to an increase in the family consent rate is an overall objective of the Community Awareness and Education Program.76 OTA advised that between 2010 and 2012, there was an increase of seven per cent in family consent rates from 54 per cent to 61 per cent. These results were below the target level of 75 per cent which has been in place since 2011–12.77
Evaluations of the campaign
3.41 Consistent with the 2010 advertising guidelines78, OTA undertook evaluations of each phase of the campaign including the extended phases. Timely and robust analysis of the progress of initiatives enables entities to identify and address potential issues with implementation and contributes to improvement processes.79 Evaluations should identify benefits realised as well as opportunities for improvement. Similarly, the 2010 advertising guidelines indicated that campaign evaluations should assess the effectiveness of government campaigns.
3.42 OTA’s evaluations assessed the effectiveness of media channels, as well as the advertisements. OTA also included two ‘lessons learned’ sections in its evaluations; one was focussed on the campaign activities and the second was focussed on the management of the campaign. OTA’s evaluations of Phase 1 and the extension of Phase 1 observed scope for improvement in respect to campaign activities and management, and identified initiatives which had worked well and should be repeated. While OTA’s evaluations for Phase 2 and the extension of Phase 2 identified initiatives which worked well, it did not identify any areas for improvement, notwithstanding the marginal improvement in outcomes reported for Phase 2 by the tracking research (refer to paragraph 3.33).
Post-campaign activities
3.43 Since July 2012, information regarding the correlation between knowledge of family members’ wishes and the consent rate has been collected through the DonateLife Audit. The 2013 DonateLife Audit results indicated that there is a higher consent rate among families who know the donation wishes of potential donors. In 2013, of the 508 requests for donation:
- 248 families knew the wishes of the potential donor and 187 (or 75 per cent) of these families provided consent for donation; and
- 132 families did not know the donation wishes of the potential donor and 59 (or 45 per cent) of these families provided consent for donation.
3.44 For the remaining 128 families, it was unknown whether the family knew the wishes of the potential donor as this information had not been collected for the DonateLife Audit. Of these 128 families, 69 (or 54 per cent) provided consent for donation.
Community Awareness Grants program
3.45 Since 2009, OTA has administered a Community Awareness Grants program.80 The objective of the grants program is to ‘assist organisations with projects or activities that contribute to improving awareness and engagement of the Australian community, the non-government sector, donor families and others involved in increasing organ and tissue donation.’81
3.46 There have been seven Community Awareness Grant rounds from November 2009 to December 2013, totalling $2.4 million. OTA conducted its eighth grant round during the course of this audit.82 The focus of the grant rounds has differed over time, as summarised in Table 3.4.
Table 3.4: Focus of grants rounds
|
Focus |
Round |
|||||||
|
|
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
|
DonateLife Week events |
|
|
Yes |
|
Yes |
Yes |
Yes |
Yes |
|
Activities and events which were targeted at culturally and linguistically diverse (CALD) communities |
|
|
|
Yes |
Yes |
Yes |
|
Yes |
|
Activities that complement OTA’s work of improving community awareness and education |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Source: ANAO analysis.
Promotion of grants
3.47 Successive grant rounds have been promoted through OTA’s website, a national media release, social media and in The Australian newspaper. All DonateLife Agencies are encouraged to promote grant rounds and OTA emails organisations in the organ and tissue sector, past grant applicants and other key stakeholders to advise them of grants rounds. OTA has also hosted teleconferences to assist applicants with completing their application form by providing an overview of the process and the type of information which is required for each criterion. Further, the guidelines encourage applicants to contact OTA or their local DonateLife Agency to discuss how to best align their proposed activity with DonateLife Week and broader DonateLife activities at a national and local level.
Grants administration
3.48 An internal audit of OTA’s grants management was completed in August 2013. The audit report noted that OTA’s grants management practices were mostly in line with the June 2013 Commonwealth Grant Guidelines and had regard to the ANAO’s Better Practice Guide on grants administration.83 One recommendation was made in relation to improving the internal policies and procedures on managing grants as well as implementing a specific training program for OTA staff involved in managing grants.84 This recommendation was agreed in part by OTA, which did not consider that the development of internal guidance was necessary given that only a small number of staff were engaged in the grant assessment process and these staff were expected to refer to the official guidance, such as the Commonwealth Grant Guidelines, issued by the Department of Finance. However, OTA did agree to an ongoing grants management training program for staff. OTA advised the ANAO that staff involved in procurement and funding activities undertake regular training, and that in 2013, all OTA staff had undertaken high level procurement and grant funding training.
3.49 As required by the Commonwealth Grants Rules and Guidelines (the grants guidelines)85, OTA has publicly available guidelines for the program. However, there remains scope for OTA to better align the program specific guidelines with OTA’s grants assessment process, to improve transparency and equity. In particular:
- OTA’s guidelines for the eighth round of grants did not indicate that DonateLife Agencies are involved in reviewing applications.
- For applications which are scored equally, OTA advised the ANAO that it reconsiders the applications in light of points of difference and this can result in a further assessment of value for money.86 This reconsideration process is not outlined in OTA’s grant guidelines.
- The grant application form provides that scope, reach and impact are all components of assessing value for money. However, scope, reach and impact are not mentioned in the program guidelines and are not defined for the benefit of applicants and assessors.
3.50 A recurring theme in the ANAO’s audits of grants administration over a number of years has been the importance of grant programs being implemented in a manner that accords with published program guidelines. Similarly, the grants administration framework was developed based, in part, on recognition that potential applicants and other stakeholders have a right to expect that program funding decisions will be made in a manner, and on a basis, consistent with the published program guidelines. The experience of the grants management process to date suggests there would be benefit in OTA better aligning assessment processes adopted with its published guidelines.
3.51 OTA advised the ANAO that it receives approximately two or three requests each year for funding outside of grants rounds, and on 14 occasions OTA has funded organisations through an unsolicited application process. On one occasion an application which was unsuccessful in a grant round was subsequently funded following receipt of a further application outside the grants process. In total, approximately $220 000 has been provided from unallocated Measure 5 funds for unsolicited applications, which were not assessed as part of the regular competitive grants assessment process. OTA also advised the ANAO that it applied its program guidelines to unsolicited applications. However, the provision of ad hoc grants funding outside the competitive public process raises issues of equity and transparency in grants administration and there would be merit in OTA advising potential applicants of all available sources of grant funding and applicable assessment processes.
Recommendation No.2
3.52 To improve transparency and equity, the ANAO recommends that OTA review its grants administration, with a particular focus on informing potential applicants of all available sources of grant funding and the assessment process applying to each source.
OTA response
3.53 Agreed.
DonateLife Week
3.54 OTA is responsible for leading and coordinating a national awareness week for organ and tissue donation. The week, called DonateLife Week, is designed to raise community awareness and support for organ and tissue donation. OTA also uses DonateLife Week to launch various initiatives and often targets its Community Awareness Grants program towards activities occurring in that week. The total cost of coordinating the week for the last three years was $122 421, plus the cost of any merchandise distributed.
3.55 OTA advised the ANAO that DonateLife Week is primarily a media and public relations campaign which is supported by sector-driven activities as a secondary focus. OTA prepares a communication plan for the Week which outlines: the aims and objectives of the week; key messages; spokespeople; media relations; corporate and community support; DonateLife Network events; and evaluation and reporting.
3.56 While events are a secondary focus for OTA, they have proven to be very successful at generating media attention. For example, in 2014 a community awareness grant recipient featured in more than twice as many media items than the combined total for lead spokespeople in the DonateLife Network.
Reach of DonateLife events
3.57 In 2014, 40 per cent of registered DonateLife Week events were in the same postcode as a DonateLife Network hospital; that is, 126 of 315 events.
Fifty-five of these events had the word ‘hospital’ in their address suggesting that they were held at hospitals. A further 33 events had the word ‘university’ in their address. When combined, this indicates that at least 28 per cent of the registered events for DonateLife Week 2014 were at a hospital or university.
3.58 OTA advised the ANAO that DonateLife Week is supported by sector-driven events and as a consequence, it would expect that a significant number of events would be organised by DonateLife Agencies and held in the same postcode as a DonateLife Network hospital. Further, one of the Community Awareness Grants was provided to conduct information stalls at universities.
3.59 There is scope for OTA to encourage a broader range of events, both within and external to the sector, to raise awareness of organ and tissue donation among the general community as well as priority groups, such as males, older people, CALD communities and Indigenous communities. Further, there is not a broad geographic reach of registered events in DonateLife Week. A map of registered events since 2011 (refer to Figure 3.1)87, indicates that there is limited reach of activities in regional and remote parts of Australia and that events are mostly held around DonateLife Network hospitals—indicated by a triangle.
Figure 3.1: Map of registered DonateLife Week events since 2011
Source: ANAO analysis.
Note: Of the events hosted in 2011, 260 were not included because location details could not be provided by OTA.
3.60 OTA commissions analysis of DonateLife Weeks, which includes high level information on media coverage in regional and metropolitan areas by state. This analysis is post-event and does not provide information regarding coverage in specific regional areas. There is scope for OTA to further consider ways to encourage events in locations where there has been limited coverage to date.
3.61 Of the 315 registered events in 2014, 110 (or 35 per cent of the total number of events) were hosted by DonateLife Network staff. Another 30 events were hosted by three community organisation Charter signatories, with one organisation responsible for 28 of these events. Of the remaining 10 community organisations which have signed the Charter, none had a registered event during DonateLife Week. Further, there were no events registered for any eye, tissue or bone banks, despite representing approximately 27 per cent of the organisations listed as Charter signatories.
3.62 OTA advised the ANAO that not all events during the week are registered despite OTA encouraging and reminding Charter signatories to do so. Nevertheless, the limited number of registered events conducted by Charter signatories in 2014 indicates that there is scope for OTA to encourage greater participation in future DonateLife Weeks among Charter signatories—now known as partners.88
3.63 Table 3.5 shows that from 2011 to 2012, DonateLife Week expanded its reach with an increase in the number of registered events. However, there was a large decrease in the number of registered events in 2013, followed by another increase in 2014. This increase is attributable to two organisations which held a combined total of 103 events. One organisation was funded through a Community Awareness Grant. Without the involvement of these two organisations, the number of events in 2014 would have been approximately the same as 2013.
Table 3.5: DonateLife Week events and coverage
|
Year |
No. of registered events |
No. of press, radio, television and online items |
Cumulative audience reach |
Total editorial value ($) |
|
2011 |
290 |
1633 |
41.6 million |
11.2 million |
|
2012 |
346 |
1580 |
51.3 million |
14.6 million |
|
2013 |
214 |
895 |
39.0 million |
18.0 million1 |
|
2014 |
315 |
1306 |
28.0 million |
10.4 million |
Source: ANAO analysis drawing on OTA records.
Note 1: OTA advised that for 2011 and 2012, the national advertising campaign resulted in high media coverage. Further, the large increase in editorial value in 2013 was due to increased levels of coverage on nationally broadcast television.
Strategy for 2014 DonateLife Week
3.64 OTA includes an overarching strategy for DonateLife Week in its National Communication Strategy and then prepares a more detailed communications plan specifically for the week. For the 2014 DonateLife Week, OTA identified three objectives:
- build on the number and reach of activities achieved in DonateLife Week 2013;
- continue the focus towards encouraging and normalising memorable family discussion of organ and tissue donation; and
- use the time frame of the week to create a sense of urgency for having the family discussion about donation wishes.
3.65 The communications plan largely focussed on media and social media as well as DonateLife Week launch events. The plan outlined targets for the frequency of use and intended outcomes for social media channels. For example, for its Facebook page, the plan outlined that OTA would make at least one post a day in the lead up to DonateLife Week and aimed to increase the number of ‘likes’ for its page by 2000.
3.66 The plan also indicated that OTA would contact key CALD communities and the broader health sector to help promote the week. Further, the communications plan outlined that OTA expected community and corporate supporters to, at a minimum, host an event encouraging people to discuss their donation wishes with family members. However, the plan did not include targets for corporate and community supporter activity.
3.67 Encouraging greater participation among corporate and community supporters may assist with generating additional media and improve the audience reach for DonateLife Week, which declined in 2014 when compared with 2013 (refer to Table 3.5). Further, it may encourage a broader range of activities which could impact a wider range of people, including people who are priority groups for OTA and who may not use social media. For example, a social media research report released in May 2014, reported that 68 per cent of people aged 65 years and older and 34 per cent of males, never use social media.89 These are both priority groups for OTA who require engagement through other communication channels. There is scope for OTA to consider setting targets in relation to corporate and community supporter activity, in the same manner as it does for social media, to focus efforts on increasing the number and reach of activities among supporters.
Measuring the effectiveness of DonateLife Week
3.68 In its communication plan, OTA identified three mechanisms to be used to evaluate and report the effectiveness of the 2014 DonateLife Week: a report commissioned by OTA in relation to CALD community engagement; a survey conducted by OTA of stakeholders; and an independent media analysis commissioned by OTA. OTA also completes a report outlining the key national activities and outcomes for DonateLife Week, as well as recommendations for future DonateLife Weeks.
3.69 The internal report outlines the results for OTA’s five communication objectives for the week which were to:
- generate high quality, positive, editorial exposure nationally for DonateLife Week 2014 in line with 2013 results;
- achieve consistent uptake of key messages and use of the donatelife.gov.au URL across media coverage;
- drive a positive community response and increase traffic to the donatelife.gov.au website, and the AODR during the course of the DonateLife Week campaign;
- effectively engage the active participation of the DonateLife Network, Community Awareness Grant recipients, DonateLife Charter signatories, and corporate and community supporters; and
- contribute to the delivery of Measure 5 of the National Reform Agenda to achieve coordinated, ongoing community awareness and education of organ and tissue donation.
3.70 Overall, the report stated that the 2014 DonateLife Week was successful in meeting these objectives, and made 32 recommendations aimed at: mainstream, ethnic and social media; the DonateLife website; key activities; engagement with CALD communities; sector and community events; materials; and supporting stakeholders. The report noted that with a limited budget and to best utilise the DonateLife Network staff, DonateLife Weeks should focus on media and public relations with a greater reliance on partnerships for community outreach.
Information and education resources
3.71 OTA has developed a range of information resources aimed at educating the community and increasing awareness of organ and tissue donation. These resources can assist with promoting consistent messages and dispelling myths. OTA provides fact sheets, a DonateLife Toolkit, a Community Speaker Guide and school curriculum resources on its website.90
3.72 OTA’s website also includes the Book of Life (the Book) which contains stories about organ and tissue donors and transplant recipients. OTA advised the ANAO that while the Book was the primary resource for raising awareness for DonateLife Weeks in 2011, 2012 and 2013; the ‘Have the Chat’ materials were the main resources in 2014.91 In 2014, the Book was used at 78 events, a decline from 189 events in 2013.
3.73 OTA has implemented an interactive version of the Book on its DonateLife website, as well as developing portable volumes of the Book. OTA has also considered special editions of the book aimed at priority groups, including people aged 65 years or older, young adults aged 18 to 29 years old and people in rural and regional areas, which have not been developed to date.
Communication with Culturally and Linguistically Diverse Communities
3.74 A priority under the national DonateLife Community Awareness and Education Program was communicating and engaging with CALD communities in Australia. Developmental research commissioned by OTA in 2010–11 reaffirmed earlier research findings from 2007 that people from CALD communities were less likely to have held a memorable family discussion on organ and tissue donation or to have made decisions on becoming organ and tissue donors.92
3.75 To guide its engagement with this audience, OTA developed the CALD Communication and Engagement Strategy 2012–15 (CALD Strategy). The aim of the strategy is to overcome barriers to discussion and decision-making about organ and tissue donation through the development and distribution of culturally appropriate information. OTA engaged a specialist agency93 to assist in the implementation of the CALD Strategy, which is focused on New South Wales and Victoria due to the large proportion of religious and cultural leaders at a national level who reside within these states, as well as the high concentration of priority CALD communities.
3.76 Based on consultation with faith and community leaders, intensivists and focus groups, OTA is targeting nine priority community groups, owing to their population size in Australia: Hindu; Muslim; Buddhist; Eastern Orthodox (focusing on Greek, Serbian and Macedonian communities); Catholic; Jewish; Antiochian; Maronite and Coptic. In addition, OTA has identified the following priority language groups: Arabic; Chinese; Greek; Hindi; Italian; Spanish; Turkish; and Vietnamese.
Approach to engage CALD communities
3.77 Beginning in 2012, OTA met with a large number of faith and community leaders from the priority communities to: provide information about organ and tissue donation and the national reform program; encourage the leader to sign a DonateLife Statement of Support for organ and tissue donation if appropriate; and discuss opportunities for distributing information about organ and tissue donation within their networks and communities. As at March 2015, 70 Statements of Support had been signed and included on the DonateLife website.94
3.78 In 2012–13, in consultation with faith and cultural leaders, OTA developed a communication education campaign, ‘DonateLife… the greatest gift’, consisting of a suite of resources including videos, brochures and religious statements of support. In 2013, the ‘DonateLife… the greatest gift’ community education campaign kit was distributed to over 500 faith and cultural organisations and over 250 health-based organisations in New South Wales and Victoria.95 The cost associated with the CALD campaign in 2012–13 and 2013–14 was $414 153 and approximately $120 000 more was allocated to the CALD campaign in 2014–15.
3.79 OTA has also produced the DonateLife-AODR brochure in 18 languages and made The Last Race educational film available in eight (subtitled) languages. To translate the DonateLife-AODR brochure into 18 languages, OTA received assistance from the then Department of Immigration and Citizenship.
3.80 The second wave of the ‘DonateLife… the greatest gift’ campaign is to develop new fact sheets and video testimonials that address misconceptions about organ and tissue donation. This process will engage faith and cultural leaders to ensure the consideration of specific cultural and religious nuances. Once this resource is developed, it will be made available to faith and cultural groups as part of planned ongoing engagement activities, community organisation partnerships and through the media. OTA has developed partnerships with 13 ethnic media organisations to generate interest and broader awareness within CALD communities, as well as helping to normalise organ and tissue donation as a topic of conversation.
Evaluation of the CALD strategy
3.81 A number of performance measures were developed by OTA to assess the impact of its engagement activities with CALD communities, including the number of CALD materials distributed at events and the number of meetings held with faith and cultural leaders. Information has been collected to inform an evaluation of the implementation of the CALD strategy, to be finalised by mid-2015.
3.82 The DonateLife Audit96, which measures data about organ donation within hospitals, also helps OTA track and measure the ethnic origin of potential donors and whether a family’s decision not to consent to donation was due to faith or cultural factors.
Indigenous Communities
3.83 The research conducted in 200797, prior to the introduction of the national reform program, identified that the low rate of donation within Indigenous communities requires particular attention as this has an impact on organ availability. Subsequent research, commissioned by OTA and conducted in 2010–11, identified barriers and issues for consideration in engaging with Indigenous audiences. Based on this research, OTA determined that engagement with Indigenous communities should be considered independently of CALD communities. To date, no strategy has been developed. OTA advised the ANAO that it intends to commence this work in 2015–16.
Effectiveness of OTA’s Community Awareness and Education Program
3.84 Table 3.6 outlines OTA’s internal performance indicators to measure the effectiveness of its Community Awareness and Education Program, as identified in its National Communication Strategy 2013–14. The results for 2013 against these indicators are also summarised in Table 3.6.
Table 3.6: National Community Awareness and Education Program performance indicators
|
Indicator |
Target |
Result for 2013 |
|
Australians have had a family discussion about organ and tissue donation1 |
70 per cent |
75 per cent |
|
Australians know their family members’ wishes about organ and tissue donation |
68 per cent |
53 per cent |
|
Number of Australians who understand the role of family consent |
74 per cent |
70 per cent |
Source: OTA internal document.
Note 1: The family discussion indicator relates to whether families had ever discussed organ and tissue donation. This indicator differs from the family discussion indicator reported in Table 3.3, which measures whether families have discussed organ and tissue donation in the past 12 months. The collection of information on whether families had ever discussed organ and tissue donation only commenced in the sixth wave of tracking research for the advertising campaign (refer Table 3.3). The result recorded as part of the sixth wave of tracking was 77 per cent.
3.85 OTA advised the ANAO that its internal performance indicators were aspirational, and were based on actual increases reported by tracking research during the initial Phase 1 advertising campaign.98 Subsequent research undertaken in 201399 has indicated that this rate of increase is unachievable without an ongoing national advertising campaign, and these indicators are being reviewed in the context of developing OTA’s National Communications Plan for 2014–18.100
3.86 While an increase in the number of registrations on the AODR is also a performance indicator for the program, OTA advised the ANAO that it does not externally report on the number of registrations as the AODR is managed by the Department of Human Services. From 30 June 2013 to 30 June 2014, there was a 1.3 per cent increase (approximately 77 800 registrations) in the number of AODR registrations. This compares with an increase of 1.6 per cent (approximately 95 200 registrations) from 30 June 2012 and 30 June 2013.101 Figure 3.2 shows that the number of Australians registered on the AODR has increased steadily since the commencement of the reform program.
Figure 3.2: Number of AODR registrations
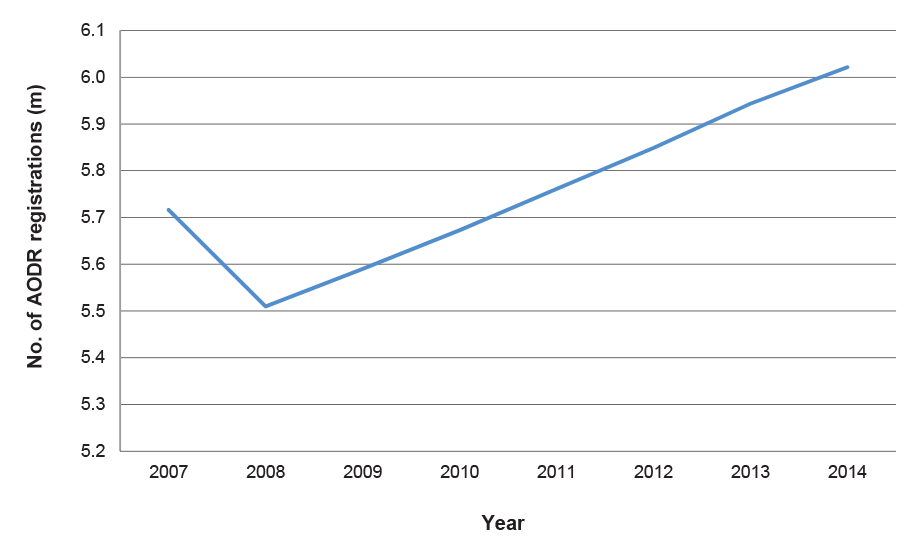
Source: ANAO analysis.
Note: The Australian Government reform program was announced on 2 July 2008 and endorsed by the Council of Australian Governments on 3 July 2008. OTA was unable to explain why there was a significant decrease in the number of registrations in 2008.
Conclusion
3.87 Under Measure 5 of the national reform program, OTA introduced a National Community Awareness and Education Program. The program included an overarching communications framework to encourage consistency of messages within the organ and tissue donation sector and provide stakeholders with access to information and resources. Thirteen community organisations which were signatories to OTA’s National Communications Charter showed high take-up rates of key elements of the Charter. There is, however, opportunity for OTA to expand the reach and impact of community awareness and education efforts by more actively facilitating collaboration between stakeholders through established forums.
3.88 The largest financial component of the National Community Awareness and Education Program was a national advertising campaign conducted from 2010 to 2012 at a cost of $13.8 million. OTA adopted an evidence-based approach for selecting the message of the campaign which focussed on promoting family discussion about organ and tissue donation.
3.89 The campaign was conducted in two phases. Tracking research indicated that while the outcomes for Phase 1 of the campaign tracked above the three benchmark indicators adopted for the campaign, overall outcomes for Phase 2 improved only marginally against two indicators and remained stable against one. Little progress was made with Phase 2 of the campaign to increase the proportion of people who indicated that they knew their family members’ wishes—a key driver of the second phase.
3.90 OTA’s Community Awareness Grants program is another component of the National Community Awareness and Education Program. Consistent with the Commonwealth Grants Rules and Guidelines, for each grant round OTA issued publicly available guidelines for applicants. However, OTA’s administration of the Community Awareness Grants Program demonstrated some misalignment between the program guidelines and assessment processes, and OTA also funded an unsuccessful applicant in a competitive grant round as part of an unsolicited application process. To improve transparency and equity, OTA should review its grants administration with a particular focus on informing potential grant funding applicants of all sources of available funding and the assessment process applying to each source.
3.91 OTA is also responsible for leading and coordinating a national community awareness week known as DonateLife Week. OTA advised the ANAO that the focus of the week is primarily on media and public relations which is supported by sector-driven events as a secondary focus. However, media analysis commissioned by OTA for the 2014 DonateLife Week indicated that events have proven to be effective at generating media attention. There is scope for OTA to encourage a broader geographic reach and range of events, including greater involvement by non-government stakeholders, which may assist in generating additional media interest during future DonateLife Weeks. Introducing targets for the level of activity undertaken by corporate and community supporters, in the same manner as it does for social media, may assist OTA to focus efforts on increasing the number and reach of activities among supporters.
3.92 OTA has developed a range of information resources, including specific resources targeted at CALD communities. OTA adopted a consultative and evidence-based approach to address the identified gap of engaging with CALD communities. OTA intends to commence work on a separate strategy for Indigenous communities in 2014–15.
3.93 In 2013, OTA advised the ANAO that it met the target for one performance indicator for the National Community Awareness and Education Program: Australians have had a family discussion about organ and tissue donation. It did not meet the targets for the other two indicators: Australians know their family members’ wishes about organ and tissue donation; and number of Australians who understand the role of family consent. OTA advised the ANAO that these targets have been deemed unachievable in the absence of another advertising campaign and it is in the process of revising them. Although OTA does not report on it, Human Services records indicate that the fourth indicator—to increase the number of AODR registrations—was also met in 2013.
4. Support for Donor Families
This chapter examines the donor family support resources and services funded by OTA.
Introduction
4.1 The National Donor Family Support Service (NDFSS) was introduced to implement Measure 6 of the reform program, which focusses on providing a nationally coordinated approach to the families of deceased donors, including support which is responsive to the needs of individual families. This measure is aimed at improving the consistency of support provided to donor families. It is expected that families of potential organ donors are offered end-of-life support, including bereavement counselling, whether or not the potential donation proceeds. For families who provide consent to donation, it is expected that additional information, ongoing support and contact be provided.
National Donor Family Support Service
4.2 Support for donor families is delivered through OTA’s NDFSS, introduced in 2011. The NDFSS is implemented through the DonateLife Network, with Donor Family Support Coordinators (DFSC) funded by OTA in each state. The aim of the NDFSS is to provide a tailored and nationally consistent program of support for donor families. From 2009–10 to 2013–14, the total cost of the NDFSS was approximately $361 000102, which included $119 000 for a national study of donor family experiences during 2010 and 2011.103
Review of information resources
4.3 To support DFSCs there is a suite of information resources targeted at donor families and transplant recipients. In 2011, OTA commissioned a review of these resources, aimed at: consolidating the materials developed by the states into a national suite of materials; and determining the most appropriate timing for providing those materials to donor families.
4.4 A research agency was engaged to conduct the review, which included a series of mini-group discussions and interviews with donor families, support staff and potential donor families.104 The review made 10 recommendations on the content of the materials tested and the timing of providing the support material to donor families. OTA implemented seven of these recommendations, but did not implement three lower-order recommendations. OTA advised the ANAO that it did not consider two of the recommendations necessary, but plans to implement the third recommendation.
4.5 Following the review, OTA developed the National Organ and Tissue Donor Family Support Service Guidelines (the support service guidelines) to define the minimum national standard of support that should be offered to donor families post-donation. However, the support service guidelines do not outline the type of support that donor families should be provided in the hospital setting. According to the National Roles and Responsibilities Guidelines, this is the responsibility of the Donation Specialist Coordinator (DSC). The National Roles and Responsibilities Guidelines indicate that there should be significant cooperation between the DSC and DFSC, including working together to meet the counselling needs of the family and following up with the family post donation.105
4.6 While the support service guidelines outline the support which should be provided to donor families post-donation, there is scope for OTA to provide enhanced guidance to the DonateLife Network in relation to the type of information and support which should be provided to donor families in the hospital setting.
Contact with families in the hospital setting
4.7 Providing information to potential donor families about brain and circulatory death was recommended in the 2011 review. This was because many of the donor families who participated in the review remembered receiving the Understanding Brain Death booklet at the hospital and had either kept it to review at a later date or to provide it to family members and friends. Potential donor families also indicated that they thought the brochure would be useful for family and friends who were not part of face-to-face discussions in the hospital context.
4.8 The usefulness of this type of information was observed in the National Study of Family Experiences of Organ and Tissue Donation conducted in 2013–14 (covering the period 2010 and 2011) by an external agency.106 Both the 2011 review and the national study also found that while written information is important, families still require verbal discussions about their specific circumstances. Providing the Understanding Death and Donation brochure, which has replaced the Understanding Brain Death brochure, to families in the hospital setting may provide the additional information some families require, particularly as it includes information about the donation process. Potentially, it could also be used as a discussion aid for describing the donation process to families.
4.9 The 2011 review also recommended that contact information for the DonateLife Agency, as well as for relevant bereavement support services, be provided to families at the hospital. The results of the national donor family study indicate that the consistency with which contact information is provided to families could be improved. Thirty-one per cent of donor family members in the study advised that they did not receive any information about bereavement support services in their area, and two-thirds of those family members indicated that they would have welcomed receiving that information. The study also found that seven per cent of family members were not offered any ongoing support. Providing contact details for support services within the hospital setting would assist those families who require access to services and could act as a prompt for offering ongoing support from DFSCs.
4.10 Further, in terms of the level of support provided to families in the hospital setting, the national study found that one-quarter of donor families were not offered the support of a social worker, counsellor or chaplain at the hospital. Further, the study found that 18 per cent of donor families had unanswered questions regarding the donation process or did not understand the donation process after discussing it with hospital staff.107 The study results indicate that there is scope to improve the consistency with which families are offered counselling as well as the type of information they are provided on the donation process. The National Roles and Responsibilities Guidelines and the support service guidelines could be revised to outline the type of support and information that should be provided to donor families in the hospital setting.
Contact with families post-donation
4.11 DSCs are expected to contact donor families within 24 to 36 hours of the donation, and DFSCs are expected to contact families two weeks after donation and six weeks after donation. There is scope for improvement in this area based on the results of the national study of donor families, which found that 22 per cent of family members did not receive a phone call from the DSC following donation. Two-thirds of these family members indicated they would have liked one.108
4.12 Of those family members contacted, 94 per cent indicated they found the contact either extremely helpful or helpful to some extent. Six per cent of family members found the contact unhelpful. Overall, 14 per cent of donor family members indicated that they did not have enough contact with their DonateLife Agency, indicating that there is an appetite for additional support.
4.13 Donor family members indicated that ongoing contact was useful for a range of reasons, including that it reassured them in their donation decision. A significant proportion of family members (30 per cent) also appreciated the contact because they learned the outcome of the donation.
4.14 Transplant recipients may choose not to correspond with donor families for a range of reasons. The support service guidelines indicate that families should be contacted within 24 to 36 hours of the donation to be advised of the donation and transplantation outcomes. Further, within two weeks of the donation, the guidelines require that donor family support resources be sent to the family. The template for the letter to accompany the resources indicates that it should include information about the transplant recipients, such as their age, gender and the organ or tissue they received.
4.15 Given the comfort it provides donor families, there would be benefit in OTA considering whether a process could be established for DFSCs to provide de-identified information about transplant outcomes in cases where transplant recipients choose not to correspond with donor families beyond the six weeks following donation.
Measuring the effectiveness of the National Donor Family Support Service
4.16 In 2009–10, there was one external indicator for donor family support, identified in the then Department of Health and Ageing’s Portfolio Budget Statement, which was: ‘Nationally consistent support offered to eligible donor families’. In 2010–11, a second external indicator was added: ‘Enhanced donor family support provided through the implementation of a nationally agreed donor family support program.’ These two indicators were discontinued by OTA in 2012–13 following a directive from the portfolio department, the then Department of Health and Ageing.109
4.17 OTA reported on achievement against the indicators in its annual reports between 2009 and 2012, as outlined in Table 4.1.
Table 4.1: Performance indicators from 2009–10 to 2011–12
|
Indicator |
Target |
2009-10 |
2010-11 |
2011-12 |
|
Percentage of nationally consistent support offered to donor families |
100 per cent |
Met1 |
Met |
Met2 |
|
Enhanced donor family support provided through the implementation of a nationally agreed Donor Family Support program |
Donor families report increasing satisfaction with support services provided according to a national audit |
N/A |
Met |
Met |
Source: ANAO analysis.
Note 1: In 2009–10, the target was 100 per cent in the Portfolio Budget Statement and was revised down to 90 per cent during the year. However, in the annual report it was inconsistently reported as 90 per cent and 100 per cent in two separate locations.110
Note 2: The target for this indicator was 100 per cent in the Portfolio Budget Statement. However, when it was reported in the annual report it was incorrectly reported as 95 per cent in one location. In any case, OTA reported it had achieved 100 per cent for the indicator. OTA advised that the target was incorrectly transcribed in the 2011–12 annual report.111
4.18 OTA reported in its annual report that in 2009–10, it had fully achieved the target for providing nationally consistent support for donor families because all DFSC positions were funded on an acting or permanent basis by 30 June 2010; a very narrow basis on which to assess a broad performance indicator of this kind.
4.19 In 2010–11 and 2011–12, OTA’s assessment of performance against this indicator was informed by the quarterly reports provided by the DonateLife Agencies, which indicated that all donor families were contacted by the DFSC and offered support services. However, the ANAO’s review of a sample of these reports indicated that there was insufficient information in those reports to confirm that consistent services had been provided to all donor families. Without receiving this information from each state and comparing it with the number of potential and actual donor families for the period, OTA was not well placed to report that it had fully achieved the target for consistently delivering services.
4.20 For the second indicator, relating to enhanced donor family support through the implementation of the NDFSS, OTA reported that the target was met in 2010–11 and 2011–12 because the family support materials had been revised. However, the target related specifically to levels of donor family satisfaction with support services, which was not measured in accordance with the target. Consequently, there was insufficient information available to report on performance against this indicator and target.
4.21 No measures have been introduced to assess the NDFSS since these indicators were discontinued. The national study of donor family experiences (refer to paragraph 4.8) does however provide a measure of the effectiveness of the support being provided to families.
4.22 The national study of donor family experiences identified areas for improvement in the quality and consistency of services as well as the clarity of information being provided to donor families. For example, staff in some states are more consistent in establishing contact with donor families. In one state 36 per cent of donor family members had not been contacted by DonateLife Network staff since donation, while in another state, all families indicated they had been contacted by DonateLife Network staff.
4.23 The Roles and Responsibilities Guidelines include high level performance measures for the positions within the DonateLife Network, including the DSC and DFSC. For example, for the DSC, one performance measure is: all families provided with adequate support and information throughout the donation process as directed by the family. More specific measures may provide OTA with greater assurance that the support service guidelines are being adhered to and that families are receiving consistent levels of support across Australia.
Conclusion
4.24 To provide a tailored and nationally consistent program of support for donor families, OTA introduced the NDFSS in 2011. To support the DFSCs, who are responsible for implementing the NDFSS, OTA revised a range of information resources for families and developed guidelines on how to provide donor family support post-donation. The guidelines could be enhanced to outline the type of support that families should be provided in the hospital setting. Further, there is scope to improve the consistency of post-donation support to families as indicated by the 2013–14 national study of donor family experiences (covering the period 2010 and 2011).
4.25 To assess the effectiveness of support services, OTA had two performance indicators in place which were discontinued in 2012–13. While OTA reported these measures as met in its Annual Reports, ANAO analysis indicated that there was insufficient information to support this result. There would be benefit in OTA developing internal performance measures to help assess the effectiveness of the NDFSS, in particular the consistency of services being provided to families.
Recommendation No.3
4.26 To improve the services provided to donor families, including those families for which consent is provided but donation does not proceed, the ANAO recommends that OTA:
- enhance the existing Roles and Responsibilities Guidelines and National Organ and Tissue Donor Family Support Service Guidelines to provide more information about the level of support families should be provided in the hospital setting; and
- in consultation with the state and territory governments, introduce internal performance measures to assess the consistency and effectiveness of donor family support services.
OTA’s response
4.27 Part (a): Agreed.
Part (b): Agreed, subject to consultation with state and territory governments.
5. Measurement and Reporting
This chapter examines OTA’s internal and external reporting, including its key performance indicators.
Introduction
5.1 As part of the national reform program, OTA is responsible for maintaining a national data and reporting system capable of tracking implementation of the nine national reform measures endorsed by the Council of Australian Governments (COAG) in 2008 and providing the public with regular and reliable information about organ and tissue donation in Australia. The key features of the system were expected to include: a new national minimum dataset; consistent data collection; performance indicators; and appropriate reporting of clinical data at both the national and state level.
Performance information
5.2 In 2009–10, OTA rolled out a data collection tool to all hospitals within the DonateLife Network to capture aggregate information at the patient level. Known as the DonateLife Hospital Performance Audit (DonateLife Audit), the tool provides for a nationally consistent method of retrospectively auditing data relating to hospital deaths in the context of organ donation.
DonateLife Audit
5.3 The data obtained by the DonateLife Audit is used to assess state and national potential for organ donation, identify missed donation opportunities and determine the consent rate for organ donation. The DonateLife Audit complements the Australia and New Zealand Organ Donation (ANZOD) Registry, which records the total number of organ donors, including those outside the DonateLife Network. The DonateLife Audit collects information from the DonateLife Network that is otherwise not collected by the ANZOD Registry, such as the number of requests made of potential donors.
5.4 The DonateLife Audit does not collect data on eye and tissue donation because of the broad and complex nature of the sector. Instead, this data is collected by the ANZOD Registry through contributions from the Australian eye and tissue banks. In 2013–14, OTA worked with the ANZOD Registry to expand the national tissue dataset and commenced reporting on this dataset in its 2013 performance report and 2013–14 annual report.
5.5 Further, the DonateLife Audit Report does not currently report on Donation after Circulatory Death (DCD), as OTA is planning to develop an appropriate definition for this category of reporting in 2015–16.112 OTA advised the ANAO that no country has yet been able to develop sufficiently accurate and robust definitions for reporting potential DCD donors. The development of a definition of the circumstances that will determine a potential DCD donor will provide greater consistency in capturing information about potential DCD donors, including the number of potential donors, request rate and consent rate. By 2017–18, OTA expects to use this information to inform strategies to increase the consent rate among families whose family member has had a circulatory death.
5.6 Overall, the DonateLife Audit has provided OTA with information to assess the effectiveness of its various initiatives including consistency in the application of the collaborative requesting approach. The information gathered through the DonateLife Audit can also be used to inform the development and delivery of OTA initiatives. For example, the DonateLife Audit collects information on why families may not provide consent for donation, which can be used to inform the FDC Workshops. OTA’s planned enhancements will further improve the usefulness of the information collected through the DonateLife Audit.
Potential donor pool
5.7 OTA has included information about the potential donor pool in its annual reports (refer to Figure 5.1). The number of potential donors is based on an extrapolation of the results reported in the September DonateLife Audit and applied to the actual number of donors as recorded by the ANZOD Registry.113 For example, in the September 2013 DonateLife Audit, the number of potential DBD donors reported was 385 and of these potential donors, there were 207 actual donors; which was a 54 per cent conversion rate. OTA applied the 54 per cent conversion rate to the actual number of donors recorded by the ANZOD Registry (391) to derive a potential donor pool of 725, which is reported in the 2013 potential donor pyramid (refer Figure 5.1).
Figure 5.1: OTA’s potential donor pyramid for 2012 and 2013
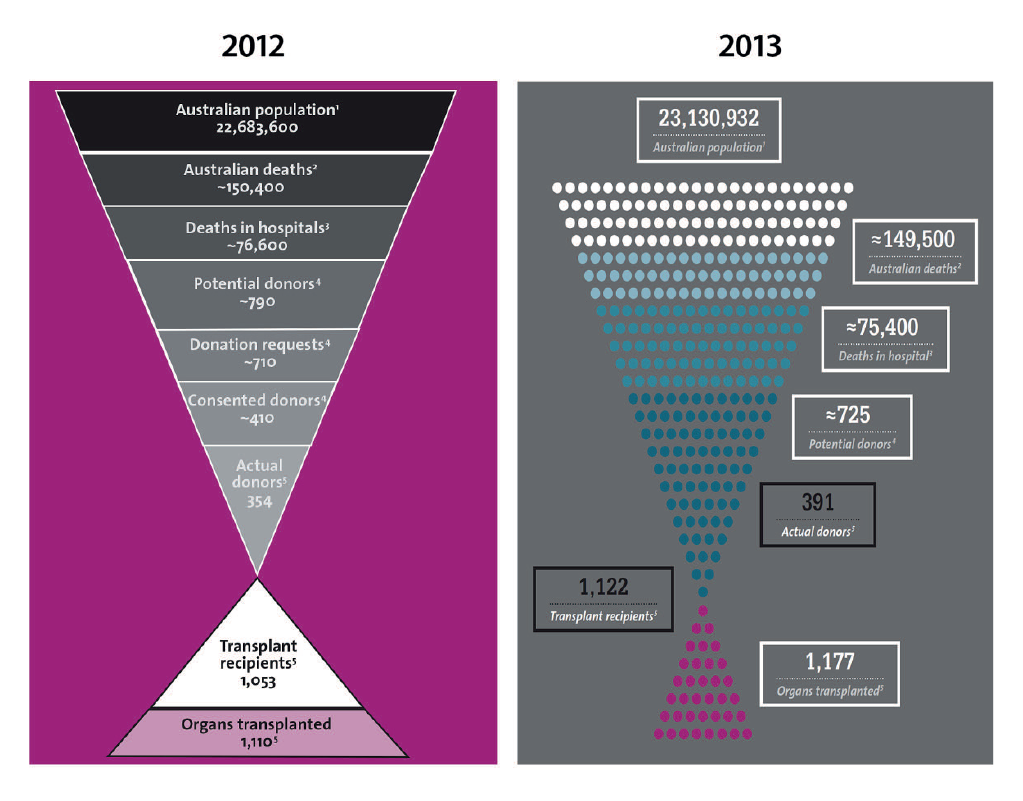
Source: OTA, 2012–13 Annual Report, p. 45; and OTA, 2013–14 Annual Report, p. 32.
5.8 OTA’s estimate of potential donors does not include:
- DCD donors, to the extent that the conversion rate only includes Donation after Brain Death (DBD) donors identified in the DonateLife Audit. As discussed in paragraph 5.5, OTA is in the process of developing a methodology for the reporting of information in relation to DCD donors; and
- potential donors located outside the DonateLife Network. OTA advised the ANAO that hospitals outside the DonateLife Network have demonstrated low potential for donation, which argues against the allocation of DonateLife Network staff to these hospitals.114
5.9 Improving the request and consent rate are key performance indicators of OTA (refer to paragraphs 5.22 to 5.23). OTA has improved its reporting from 2012 to 2013 by excluding the request rate in the 2013 pyramid, which had led to discrepancies in its reporting. Previously, there was a difference between the request rate reported in the pyramid and the request rate reported against the target key performance indicator in the 2012–13 annual report. The difference arose because, against the key performance indicator, OTA only reports on DBD using the DonateLife Audit data.
5.10 Enhancing the DonateLife Audit to record DCD would further improve the accuracy of the estimated figures reported in OTA’s potential donor pyramid. However, OTA will not be able to report accurately on the actual potential donor pool as there will be potential donors outside the DonateLife Network who are not identified and recorded by the DonateLife Audit.
Internal reporting
5.11 The performance of each state and territory (state) is monitored by OTA through a standardised reporting framework outlined in individual state funding agreements. DonateLife Agencies are required to submit biannual progress reports in accordance with a template developed by OTA, reporting on progress against the nine reform measures and any adverse events.115 The reports are reviewed by OTA and key issues are discussed with the DonateLife Agencies.
5.12 OTA provides monthly reports to the DonateLife Network, as well as the Advisory Council and the Department of Health, on organ donation and transplantation performance. The data is collected from the ANZOD Registry, and re-presented as trend information. OTA also provides the Australian Health Ministers’ Advisory Council with annual progress reports on implementation of the national reform program.
External reporting
5.13 Since its establishment, OTA has reported publicly on its progress in implementing the national reform program, as well as broader measures associated with organ and tissue donation. Information has been provided in OTA’s annual reports and through a series of biannual performance reports available on its website.116
Annual Reports
5.14 OTA published its first annual report in 2008–09, and has published six in total. In addition to detailing the activities undertaken by the DonateLife Network in delivering the national reforms, the annual reports include performance information on the nine reform measures. The reports also provide trend information, comparison data and information on developments in international organ and tissue donation, and Australia’s potential donor population.
Number of donors
5.15 Since the start of the reform program in 2009, there has been an increase in the number of Donation after Brain Death (DBD) and Donation after Circulatory Death (DCD) donors, as illustrated in Figure 5.2. In 2014, there was an overall decrease in the number of donors compared with 2013 from 391 to 378 donors.
Figure 5.2: Number of donors by DBD and DCD
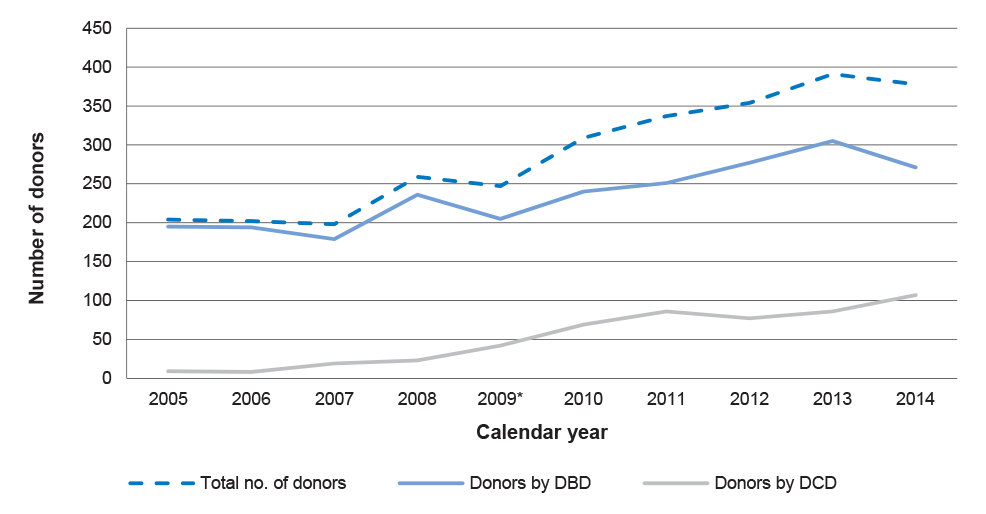
Source: ANAO analysis based on ANZOD Registry information.
Note*: The national reform program was announced by the Australian Government and endorsed by the Council of Australian Governments in 2008. The reform program commenced in 2009.
5.16 Measure 1 of the national reform program included the development of clinical protocols regarding the organ donation process, organ allocation and waiting list management. In July 2010, OTA assumed responsibility for implementing a DCD clinical practice protocol developed by the National Health and Medical Research Council. In its 2010–11 annual report, OTA reported that it distributed a national implementation plan to assist the states to implement the protocol. OTA also advised the ANAO that it had been working with states to identify opportunities for increasing the uptake and consistency of DCD practice. These efforts may have contributed to the increase in the number of DCD donors.
Donors per million population
5.17 Included in OTA’s annual reports is information about Australia’s deceased donor per million population (dpmp) rate. As discussed in Chapter 1, dpmp is a common measure, which is also used by OTA to compare performance across the states and to compare Australian performance with other countries.
5.18 Annual national and state indicative dpmp targets have been in place since the beginning of 2011, in line with the findings of the Mid-Point Implementation Review Report (refer to paragraphs 1.18 and 1.19). OTA developed state and national indicative growth trajectories and annual targets to achieve a national target of 25 dpmp by 2018. States’ performance against annual targets is reported internally through monthly data reports. The annual dpmp rate is reported externally in OTA’s performance reports.
5.19 As illustrated in Figure 5.3, OTA has reported that up to 2013, there have been annual increases in Australia’s dpmp since the commencement of the reform program. In 2014, there was a slight decline in the dpmp rate from 16.9 in 2013 to 16.1 dpmp.
Figure 5.3: Australia’s donor per million population
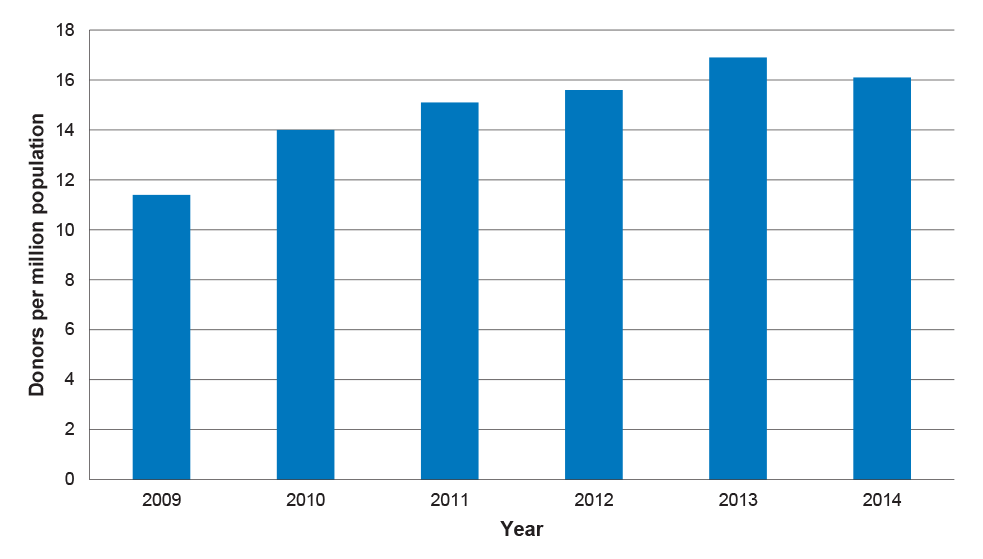
Source: OTA, Performance Report 2014 [Internet], OTA, Canberra, 2014, available from:
<http://www.donatelife.gov.au/sites/default/files/OTA%202014%20Performance%20Report%20Jan%202015%20FINAL.pdf> [accessed February 2015].
5.20 OTA advised the Senate Community Affairs Legislation Committee in February 2015 that the decline was partly attributable to the variability of donation outcomes between states and territories. OTA also highlighted a lack of consistency between states and territories in applying the Family Donation Conversation training, which OTA considered had adversely affected the family consent rate (refer to paragraphs 2.23 to 2.25). Figure 5.4 illustrates donor per million population outcomes for states and territories in 2014.
Figure 5.4: Donor per million population by state in 2014
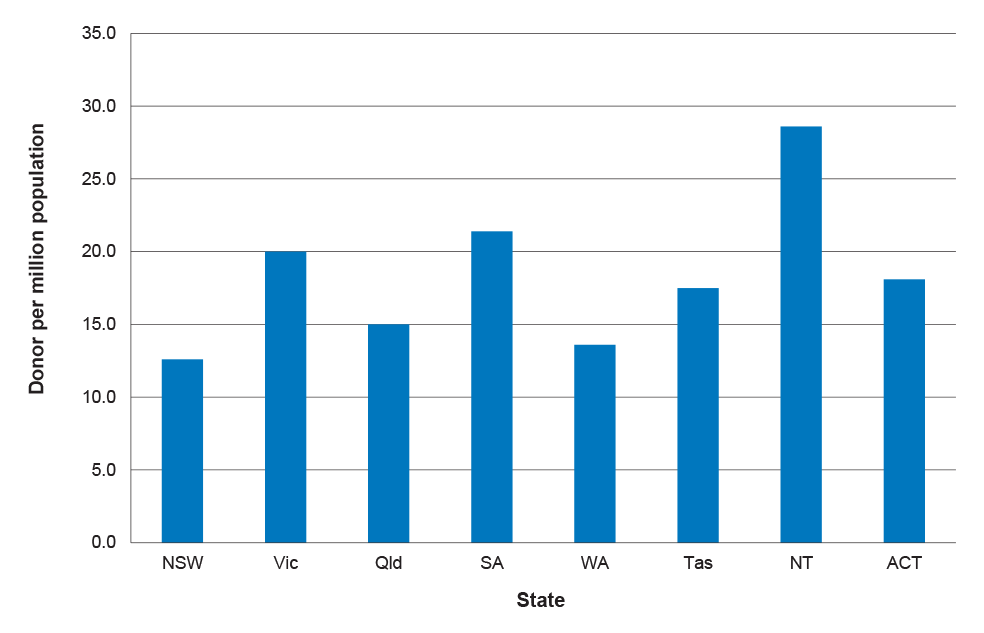
Source: Derived from: OTA, Performance Report 2014 [Internet], OTA, available from: http://www.donatelife.gov.au/sites/default/files/OTA%202014%20Performan… [accessed March 2015].
Performance framework
5.21 OTA’s annual reports report against the performance framework outlined in the Portfolio Budget Statement for the Health Portfolio. In 2013–14, OTA had one outcome: ‘Improved access to organ and tissue transplants, including through a nationally coordinated and consistent approach and system’, and one program: ‘A nationally-coordinated system for organ and tissue donation for transplantation’.117 OTA reported in its 2013–14 annual report that it had met the program’s four qualitative deliverables, as summarised in Table 5.1. One of the deliverables, highlighted in grey, relates to OTA’s community awareness, education and social marketing activities.
Table 5.1: Program 1.1: Objectives and qualitative deliverables
|
Program objective |
Qualitative deliverable |
2013–14 |
|
Implement an Organ and Tissue Donation Clinical Governance Framework |
Implement the elements of the Clinical Governance Framework in DonateLife hospitals across Australia by 30 June 2014 |
Met |
|
Integrate the eye and tissue network into the DonateLife Network |
Develop a national education program for the eye and tissue sector based on a combination of online and face-to-face learning modules, national practical competencies and a self-paced training module |
Met |
|
Raise community awareness and stakeholder engagement across Australia |
Conduct community awareness and education activities on organ and tissue donation, in partnership with sector and community organisations |
Met |
|
Implement an Electronic Donor Record |
Implement an Electronic Donor Record |
Met |
Source: 2013-14 Portfolio Budget Statement, Health and Ageing portfolio, p. 354; and Australian Organ and Tissue Donation and Transplantation Authority, 2013–14 Annual Report.
5.22 There are two quantitative key performance indicators for the OTA program (Program 1.1), which first appeared in the 2012–13 Portfolio Budget Statement for the then Health and Ageing portfolio:
- rate of request by hospital staff to families for organ and tissue donation (100 per cent); and
- rate of family consent to organ and tissue donation (75 per cent).
5.23 For 2013–14, OTA did not meet these targets, reporting the following results against the performance indicators:
- request rate: 96 per cent against a target of 100 per cent;
- consent rate: 62 per cent against a target of 75 per cent; and
- conversion rate: 53 per cent against a target of 70 per cent.118
Performance reports
5.24 OTA provides reports on its website relating to performance in implementing the national reform program. The reports include information on the number of donors, number of transplant recipients and number of organs transplanted. The reports have been prepared on a six-monthly basis since 2010 and supplementary reports are also prepared on an ad hoc basis. OTA did not produce a six-monthly report during 2014, instead publishing an annual report in January 2015. OTA advised the ANAO that in future it will only produce annual reports, and will assess the need for periodic reports taking into account agency resources and priorities.
5.25 The content of reports has varied over time. For example, the family consent rate has not been included since the first annual report in 2010. However, additional information has been included in subsequent reports, such as information about eye and tissue donation.
5.26 OTA’s performance reports have not included information about the number of registrations on the AODR. OTA advised the ANAO that it is not responsible for administering the AODR and does not report on the register. Notwithstanding the administrative arrangements for the AODR, the level of registrations is a relevant consideration in assessing Australia’s overall performance on organ and tissue donation. Further, registering on the AODR is now a key message of OTA’s National Community Awareness and Education Program. Against this background, there would be merit in OTA reporting on the number of AODR registrations in its performance reports, to provide a holistic view of the state of play in Australia.
Conclusion
5.27 Consistent with the national reform program, OTA introduced a national data collection tool known as the DonateLife Audit. It is limited to the DonateLife Network and does not collect information about eye and tissue donation. Further, while the DonateLife Audit reports information on DBD, it does not report information about DCD. This limits OTA’s capacity to report on the total number of potential donors, the request rate and the consent rate. Nevertheless, the DonateLife Audit provides information that can be used to assess the effectiveness of OTA’s various initiatives, and OTA’s planned enhancements will further improve the usefulness of the information collected.
5.28 OTA reports externally on its progress in implementing the national reform program. Indicators such as dpmp and number of donors have improved since the commencement of the national reform program but declined slightly in 2014. Further, OTA is not achieving the targets set for the program’s quantitative performance indicators. OTA’s performance reports could be improved by including information on the number of AODR registrations to provide a more holistic view of the impact of the national reform program.
Appendices
Appendices
Please refer to the attached PDF for the Appendices:
- Appendix 1: Entity Response
Abbreviations
|
ANAO |
Australian National Audit Office |
|
ANZOD |
Australia and New Zealand Organ Donation (Registry) |
|
AODR |
Australian Organ Donor Register |
|
CALD |
Culturally and linguistically diverse |
|
CICM |
College of Intensive Care Medicine |
|
COAG |
Council of Australian Governments |
|
DBD |
Donation after Brain Death |
|
DCD |
Donation after Circulatory Death |
|
DFSC |
Donor Family Support Coordinators |
|
dpmp |
Deceased donors per million population |
|
DSC |
Donation Specialist Coordinator |
|
FDC |
Family Donation Conversation (Workshop) |
|
ICC |
Independent Communications Committee |
|
NDFSS |
National Donor Family Support Service |
|
OTA |
Australian Organ and Tissue Donation and Transplantation Authority |
Glossary
|
Australian Organ Donor Register |
The national register for people to record their decision about becoming an organ and tissue donor for transplantation after death. |
|
Collaborative requesting model |
A team-based approach involving the intensive care specialist, a DonateLife trained requestor and relevant health professionals raising the opportunity for organ and tissue donation with families once they understand that death has occurred or is expected to occur. |
|
Consent rate |
Number of consents as a proportion of the number of requests made of potential donors. |
|
Conversion rate |
Number of brain-dead donors as a proportion of the number of potential donors with confirmed or probable brain death. |
|
Designated requestor model |
A team-based approach involving a DonateLife trained requestor and relevant health professionals raising the opportunity for organ and tissue donation with families once they understand that death has occurred or is expected to occur. |
|
Donation after brain death |
Organ donation after brain death has been determined on the basis of irreversible cessation of all brain function. |
|
Donation after circulatory death |
Organ donation after circulatory death has been determined on the basis of irreversible cessation of blood circulation. |
|
DonateLife Agencies |
Organ and tissue donation agencies that are responsible for implementing the national reform program in their respective state or territory. These agencies employ specialist staff in organ and tissue donation coordination, professional education, support for donor families, communications, and data and audit roles. |
|
DonateLife Audit |
Nationally consistent audit on potential and actual donor activity used to improve clinical practice in organ donation. |
|
DonateLife Network |
National network of organ and tissue donation agencies and hospital-based staff, focused on increasing organ and tissue donation. |
|
Deceased donors per million population |
The most common measure used for international comparisons of performance in organ and tissue donation. |
|
Hospital-based staff |
Specialist hospital staff, including donation specialist doctors, nurses and nursing coordinators, primarily funded by the Australian Government as part of the DonateLife Network. |
|
Intensivist |
Intensive care medical specialist staff who are involved in the assessment, resuscitation and ongoing management of critically ill patients with life-threatening single and multiple organ system failure. |
|
National reform program |
The nine measures that describe the key strategies of the Australian Government’s 2008 World’s Best Practice Approach to Organ and Tissue Donation for Transplantation. |
|
Request rate |
Number of requests of potential donors as a proportion of the total number of potential donors. |
Footnotes
1 The framework for ‘informed consent’ is established by state and territory Human Tissue Acts. The alternative to ‘informed consent’ is ‘presumed consent’, an opt-out model which presumes consent by adults to donate their organs and tissue in the event of their death, unless they advise otherwise.
2 The Australian Organ Donor Register is administered by the Australian Government Department of Human Services.
3 National Health and Medical Research Council, Organ and Tissue Donation After Death, For Transplantation: Guidelines for Ethical Practice for Health Professionals, NHMRC, Canberra, 2007, pp. 33-34.
4 The Taskforce reported in January 2008 that there was no clear correlation between models of ‘presumed consent’ and better performance in the rate of organ donation and therefore did not recommend changes to Australia’s consent framework. National Clinical Taskforce on Organ and Tissue Donation, Final Report: Think Nationally, Act Locally, Department of Health and Ageing, Canberra, 2008.
5 K Rudd (Prime Minister) and N Roxon (Minister for Health and Ageing), ‘$136.4 million national plan to boost organ donation and save lives’, media release, Parliament House, Canberra, 2 July 2008.
6 The Australian Organ and Tissue Donation and Transplantation Authority (OTA) was established in January 2009.
7 Measure 1 was the introduction of ‘a nationally coordinated approach to organ procurement based on world’s best practice models.’ This included the establishment of a new, independent authority ‘to provide national leadership to the organ and tissue sector and to drive, implement and monitor national reform initiatives and programs.’ Commonwealth of Australia, A world’s best practice approach to organ and tissue donation for Australia: overview, Commonwealth of Australia, Canberra, 2008, p. 3.
8 The DonateLife brand is an Australian Government program brand developed by OTA for the organ and tissue sector.
9 These 72 hospitals were chosen by respective states as having the greatest potential for donation. A small number of hospitals outside the DonateLife Network also have the potential for donation. The addition of new hospitals to the network is reviewed on a case-by-case basis.
10 Relevant frameworks applied to assess this criterion included the Guidelines on Information and Advertising Campaigns by Australian Government Departments and Agencies and the Commonwealth Grants Rules and Guidelines.
11 The Australasian Donor Awareness Program has been delivered in Australia since 1994 and is intended to provide participants with a greater understanding of organ donation and the skills to sensitively conduct conversations with families about organ and tissue donation.
12 The core FDC Workshop provides detailed theoretical information about acute grief and communicating with families to support an informed decision in relation to organ and tissue donation. The practical FDC Workshop complements the core FDC Workshop by providing the opportunity to participate in targeted role plays. In response to a review of the Professional Education Package undertaken in 2013, which identified some duplication with the College of Intensive Care Medicine (CICM) training, OTA was revising the Package in the course of the audit. OTA advised the ANAO that the Australasian Donor Awareness Program will be replaced with the Introductory Donation Awareness Training Workshop in May 2015.
13 Intensivists are medical specialist staff involved in providing intensive care medicine, which includes the assessment, resuscitation and ongoing management of critically ill patients.
14 The collaborative requesting model involves a team-based approach involving the intensive care specialist, a DonateLife trained requestor and relevant health professionals raising the opportunity for organ and tissue donation with families once they understand that death has occurred or is expected to occur.
15 The designated requestor model involves a team-based approach involving a DonateLife trained requestor and relevant health professionals raising the opportunity for organ and tissue donation with families once they understand that death has occurred or is expected to occur.
16 Four waves of tracking research were conducted during Phase 1 of the campaign and its extension (Waves 1 to 4), and two further waves of research were conducted during Phase 2 and its extension of the campaign (Waves 5 to 6).
17 OTA advised the ANAO that the targets for indicators one to three were being revised at the time of the audit as research undertaken in 2013 indicated that they were not achievable without another advertising campaign.
18 A target has not been set for this indicator. OTA does not report on AODR registrations. This information was sourced from: Department of Human Services, Australian Organ Donor Register (AODR) Historical Statistics [Internet], DHS, available from <http://www.humanservices.gov.au/ corporate/statistical-information-and-data/australian-organ-donor-register-statistics/australian-organ-donor-register-historical-statistics> [accessed 16 March 2015].
19 While OTA’s National Organ and Tissue Donor Family Support Service Guidelines indicate that the donor’s family should be contacted within 24 to 36 hours of donation, OTA advised the ANAO that in practice, the primary contact is with the senior next of kin. Respondents to the national study of donor families included both the donor’s senior next of kin and other family members. OTA advised the ANAO that the survey respondents who indicated that they had not been contacted, may have been family members other than the senior next of kin.
20 The two indicators were: nationally consistent support offered to donor families; and enhanced donor family support provided through the implementation of a nationally agreed donor family support program.
21 The DonateLife Hospital Performance Audit (DonateLife Audit) was introduced by OTA in 2009–10. It provides for a nationally consistent method of retrospectively auditing data relating to hospital deaths in the context of organ donation.
22 The DonateLife Audit does not collect data on eye and tissue donation because of the broad and complex nature of the eye and tissue donation sector. Instead, this data is collected by the ANZOD Registry through contributions from the Australian eye and tissue banks.
23 In the decade prior to the launch of the national reform program, Australia’s rate of dpmp remained relatively constant at around 10 dpmp. Following annual increases, this figure rose to 16.9 dpmp in 2013 and then declined somewhat to 16.1 dpmp in 2014.
24 For 2013–14, OTA reported a: 96 per cent request rate against a target of 100 per cent; 62 per cent consent rate against a target of 75 per cent; and 53 per cent conversion rate against a target of 70 per cent.
25 The Taskforce reported in January 2008 that there was no clear correlation between models of ‘presumed consent’ and better performance in the rate of organ donation and therefore did not recommend changes to Australia’s consent framework. National Clinical Taskforce on Organ and Tissue Donation, Final Report: Think Nationally, Act Locally, Department of Health and Ageing, Canberra, 2008.
26 K Rudd (Prime Minister) and N Roxon (Minister for Health and Ageing), ‘$136.4 million national plan to boost organ donation and save lives’, media release, Parliament House, Canberra, 2 July 2008.
27 The Australian Organ and Tissue Donation and Transplantation Authority (OTA) was established in January 2009.
28 The framework for ‘informed consent’ is established by state and territory Human Tissue Acts. The alternative to ‘informed consent’ is ‘presumed consent’, an opt-out model which presumes consent by adults to donate their organs and tissue in the event of their death, unless they advise otherwise.
29 This figure includes 24 554 registered objections.
30 National Health and Medical Research Council, Organ and Tissue Donation After Death, For Transplantation: Guidelines for Ethical Practice for Health Professionals, NHMRC, Canberra, 2007, pp. 33-34.
31 Overall, Australia was ranked 28th in the world in 2009 (11.3 dpmp) and 20th in the world in 2013.
32 OTA was a prescribed agency under the Financial Management and Accountability Act 1997. From 1 July 2014, OTA is subject to the Public Governance, Performance and Accountability Act 2013. The Department of Health was known as the Department of Health and Ageing prior to a machinery of government change in September 2013.
33 These reports were biannual from 2011 to 2013. OTA advised the ANAO that it will prepare an annual report for 2014 and make an assessment year-to-year regarding whether it will prepare biannual reports.
34 The DonateLife brand is an Australian Government program brand developed by OTA for the organ and tissue sector.
35 These 72 hospitals were chosen by states as having the greatest potential for donation, meaning there remain a small number of hospitals outside of the DonateLife Network with the potential for donation. The addition of new hospitals to the network is reviewed on a case-by-case basis.
36 These guidelines were revised in 2014.
37 Clinical protocols guide national clinical practice by specifying the eligibility criteria for entry onto organ transplant waiting lists; donor suitability criteria for organ allocation for transplantation; and the organ allocation protocols for determining transplant recipients.
38 Australian Healthcare Associates, Organ and Tissue Donation Reform Package: Mid-Point Review Report, AHA, Melbourne, 2011.
39 Relevant frameworks applied to assess this criterion included the Guidelines on Information and Advertising Campaigns by Australian Government Departments and Agencies and the Commonwealth Grants Rules and Guidelines.
40 These measures are discussed in paragraphs 1.6 to 1.8.
41 OTA is also developing training specifically for the eye and tissue donation sector, which has not been reviewed as part of this audit.
42 The core FDC Workshop provides detailed theoretical information about acute grief and communicating with families to support an informed decision in relation to organ and tissue donation. The practical FDC Workshop complements the core FDC Workshop by providing the opportunity to participate in targeted role plays.
43 The Introductory Donation Awareness Training workshop will replace the Australasian Donor Awareness Program and is discussed at paragraph 2.6. The advanced training was scheduled for introduction in 2015. OTA also engaged a training provider to prepare an e-learning package to accompany the FDC Workshops at a cost of $42 524.
44 Intensivists are medical specialist staff involved in providing intensive care medicine, which includes the assessment, resuscitation and ongoing management of critically ill patients.
45 Including 13 medical and 54 general workshops.
46 The $47 800 procurement involved a direct source process. OTA considered that this direct source approach was consistent with the 2008 Commonwealth Procurement Guidelines as the procurement was below the $80 000 threshold for open tender. Department of Finance and Deregulation (now the Department of Finance), Commonwealth Procurement Guidelines, DoFD, Canberra, 2008, p. 30.
47 This procurement of up to $74 000 also involved a direct source process. OTA considered that this direct source approach was consistent with the 2008 Commonwealth Procurement Guidelines as the procurement was below the $80 000 threshold for open tender. Department of Finance and Deregulation, Commonwealth Procurement Guidelines, DoFD, Canberra, 2008, p. 31.
48 Under the first contract, the Institute also developed an e-learning module to accompany the training developed by the Australian provider. It was deemed to be unsuitable for the Australian audience and consequently, was not introduced. Consequently, OTA has engaged another provider to develop FDC e-learning training at a cost of $42 524 (refer to Footnote 43).The Institute also conducted a quality assurance review of the training developed by the Australian provider.
49 OTA executed two contracts with the Institute and three variations. To date, the total value of these contracts has been US$795 144. OTA reported the contracts and variations on AusTender, which provides for centralised reporting on Australian Government contracts.
50 These improvements involved combining and shortening two components of the training to enable more opportunities for the participants to practice the skills they were learning.
51 OTA consulted with the DonateLife State Medical Directors and Agency Managers in July 2011 to determine the most appropriate requesting model to promote in the training and decided on the collaborative requesting model. The collaborative requesting model involves a team-based approach involving the intensive care specialist, a DonateLife trained requestor and relevant health professionals raising the opportunity for organ and tissue donation with families once they understand that death has occurred or is expected to occur. The model promotes a ‘balanced’ approach to communicating with families, which includes explaining the positive aspects of donation while reassuring families that any decision they make will be supported. This approach differs from the ‘neutral’ approach to explaining organ and tissue donation previously adopted in most hospitals, which did not involve discussing the positive aspects of donation.
52 Discussed in paragraph 2.5.
53 CICM trainees registered from 1 January 2015 are required to complete the FDC training.
54 This study was undertaken in 2013–14 and released by OTA in 2014. Organ and Tissue Authority, National study of family experiences of organ and tissue donation: Wave 1–2010 and 2011, OTA, 2014, Canberra.
55 The Jurisdictional Advisory Group is the key governance committee for the DonateLife Network. It comprises State Medical Directors and state health department representatives.
56 The DonateLife Hospital Performance Audit (DonateLife Audit) was introduced by OTA in 2009–10. It provides for a nationally consistent method of retrospectively auditing data relating to hospital deaths in the context of organ donation.
57 The designated requestor model involves a team based approach involving a DonateLife trained requestor and relevant health professionals raising the opportunity for organ and tissue donation with families once they understand that death has occurred or is expected to occur.
58 The nine COAG reform measures are listed at paragraph 1.4 of this audit report.
59 Commonwealth of Australia, A world’s best practice approach to organ and tissue donation for Australia: overview, Commonwealth of Australia, Canberra, 2008, p. 8.
60 The national calendar of events includes events to be conducted by government and non-government stakeholders in the organ and tissue sectors. It enables Charter signatories to plan and implement complementary localised community awareness and education.
61 This research was commissioned by the then Department of Health and Ageing to inform a communications strategy about organ and tissue donation.
62 The advertising agencies were sourced from an Australian Government multi-use list. This procurement was not examined in detail by the ANAO.
63 The testing involved 25 group discussions and 15 in-depth interviews. Testing was undertaken in seven locations (including four metropolitan and three regional centres) across four states.
64 This value for money assessment included three key criteria: achieving the requirement; tenderer’s capacity and infrastructure; and whole of projects costs.
65 This was the same research agency engaged to carry out the original testing of campaign materials. The ANAO did not examine the procurement in detail.
66 OTA engaged an agency to undertake a benchmark survey and six waves of tracking research throughout the campaign.
67 Department of Finance and Deregulation, Guidelines on Information and Advertising Campaigns by Australian Government Departments and Agencies, Department of Finance and Deregulation, Canberra, 2010, p. 8.
68 There were two other similar suggestions which were made in relation to the second round of testing: using a different image for the print advertisement and shortening the internet banner.
69 The third round of testing was focussed on using a potential alternate tagline of ‘Of course’ instead of ‘OK’.
70 The first round was undertaken in three locations which were Sydney, Brisbane and Bendigo. The second round of testing was only conducted in Sydney and Brisbane.
71 The ICC was appointed to provide advice to Financial Management and Accountability Act 1997 (FMA Act) agencies in relation to proposed advertising campaigns valued at more than $250 000. The ICC was disbanded with the release of interim guidelines in November 2013, which did not make provision for third party scrutiny and advice on campaign compliance with government guidelines. The Australian Government announced in December 2014 that from 1 February 2015, the ICC would be re-established.
72 Six Chief Executive certifications were submitted to the ICC dated: 18 May 2010, 9 May 2011, 17 December 2010, 1 March 2011, 1 December 2011 and 1 November 2010.
73 Department of Finance and Deregulation, Guidelines on Information and Advertising Campaigns by Australian Government Departments and Agencies (March 2010), Department of Finance and Deregulation, Canberra, 2010, p. 9.
74 Specifically, Regulations 9 and 13 which, at that time, established the financial framework requirements for the commitment of public money.
75 The term ‘wave’ is used to refer to the six rounds of tracking research conducted.
76 OTA advised that this family consent indicator is influenced by both the clinical reform agenda and other community awareness and education activities.
77 The target level was previously 70 per cent. In 2011, OTA estimated that if 75 per cent of families agreed to organ donation, Australia could achieve a deceased donor per million population (dpmp) rate of 25 dpmp.
78 Department of Finance and Deregulation, op cit., 2010, p. 9.
79 ANAO Better Practice Guide—Successful Implementation of Policy Initiatives, October 2014, p. 62.
80 Under section 11 (1) (g) of the Australian Organ and Tissue Donation Transplantation Authority Act 2008, OTA’s Chief Executive Officer can make a grant of financial assistance, on behalf of the Australian Government, in relation to organ or tissue donation and transplantation matters. The Minister for Health is advised of the outcome of the relevant grant round, including grant recipients and unsuccessful grant applications.
81 OTA, internal document.
82 OTA advised the ANAO that 22 organisations received total funding of $462 064 in the eighth grant round. The grant assessment and allocation process applied in this grant round was not reviewed in detail by the ANAO.
83 ANAO Better Practice Guide—Implementing Better Practice Grants Administration, December 2013.
84 The internal audit did not specify the grant rounds assessed.
85 Department of Finance, Commonwealth Grants Rules and Guidelines, Department of Finance, 2014, Canberra, p. 20. The grants rules and guidelines replaced the Commonwealth Grant Guidelines, following the introduction of the Public Governance, Performance and Accountability Act 2013.
86 The ANAO also identified in two rounds, two applications which scored higher than other funded applications but which were not funded.
87 Event locations are shaded in yellow.
88 As discussed in paragraph 3.7, OTA introduced the DonateLife Stakeholder Engagement Framework in 2014 to replace the National Communication Framework and Charter. The Stakeholder Engagement Framework outlines a new partner framework.
89 Sensis Pty Ltd, Yellow Social Media Report [Internet], Sensis Pty Ltd, Melbourne, 2014 <https://www.sensis.com.au/content/dam/sas/PDFdirectory/Yellow-Social-Media-Report-2014.pdf> [accessed February 2015].
90 OTA’s website also includes video stories of donor families and transplant recipients, and other multimedia products.
91 These materials included a ‘Have the Chat’ video, printed materials and merchandise.
92 The 2007 research was commissioned by the then Department of Health and Ageing to inform a communications strategy about organ and tissue donation. It is also referred to in the discussion about the development of the advertising campaign earlier in this Chapter.
93 This agency was engaged using a government multi-use list. The ANAO did not examine this procurement in detail.
94 There are also six position statements and rulings from different religious and cultural leaders.
95 In 2013–14, over 100 000 CALD resources were distributed to stakeholders, based on agreed allocations.
96 The DonateLife Hospital Performance Audit (DonateLife Audit) was introduced by OTA in 2009–10. It provides for a nationally consistent method of retrospectively auditing data relating to hospital deaths in the context of organ donation.
97 Refer to paragraph 3.15.
98 The campaign is discussed in paragraphs 3.15 to 3.43 of this audit report.
99 This research was part of annual tracking research commissioned by OTA and undertaken by a research agency in 2013.
100 OTA advised the ANAO that it intends to finalise this plan by the end of 2014–15. OTA also advised the ANAO that the revised indicators will be informed by the national study of donor family experiences and the DonateLife Audit, as well as the OTA’s market research.
101 Department of Human Services, Australian Organ Donor Register (AODR) Historical Statistics [Internet], DHS, available from <http://www.humanservices.gov.au/corporate/statistical-information-and-data/australian-organ-donor-register-statistics/australian-organ-donor-register-historical-statistics> [accessed 16 March 2015].
102 This figure does not include the resource costs of the DonateLife staff.
103 Organ and Tissue Authority, National Study of Family Experiences of Organ and Tissue Donation: Wave 1–2010 and 2011, OTA, 2014, Canberra.
104 Of the donor families, 34 family members from 17 donor families completed surveys for the study. The research agency was engaged following a Request for Quotation process involving three providers. This procurement was not examined in detail by the ANAO.
105 The National Roles and Responsibilities Guidelines, issued by OTA, outline the responsibilities of the positions within the DonateLife Network.
106 Organ and Tissue Authority, National Study of Family Experiences of Organ and Tissue Donation: Wave 1–2010 and 2011, OTA, 2014, Canberra.
107 Included in this figure of 18 per cent are: 16 per cent of survey participants who indicated that they were informed but still had some questions; and two per cent of survey participants who indicated that they did not have a good understanding of the donation process. The remaining 82 per cent of participants indicated that they were well informed.
108 While the support service guidelines indicate that the donor’s family should be contacted within 24 to 36 hours of donation, OTA advised the ANAO that in practice, the primary contact is with the senior next of kin. Respondents to the national study of donor families included both the donor’s senior next of kin and other family members. OTA advised the ANAO that the survey respondents who indicated that they had not been contacted, may have been family members other than the senior next of kin.
109 The directive was to reduce the number of deliverables and key performance indicators to four for each program.
110 Department of Health and Ageing, Australian Organ and Tissue Donation and Transplantation Authority: Agency Resources and Planned Performance, DoHA, 2009, Canberra, p. 442 and Organ and Tissue Authority, 2009–10 Annual Report, OTA, 2010, Canberra, pp. 33 and 44.
111 ibid., p. 512 and ibid., p. 45.
112 Donation after circulatory death (DCD) occurs after circulatory death has been determined on the basis of irreversible cessation of blood circulation. Donation after brain death (DBD) occurs after brain death has been determined on the basis of irreversible cessation of all brain function.
113 The September DonateLife Audit report includes information from January to September for the relevant year.
114 In 2014, 97 per cent of actual donors were from the DonateLife Network and three per cent were from outside the Network.
115 Adverse events can include organs for transplantation lost during transportation, or the transmission of infectious diseases.
116 OTA, National Performance Data [Internet], OTA, Canberra, 2014, available from http://www.donatelife.gov.au/national-performance-data [accessed October 2014].
117 Department of Health and Ageing, Australian Organ and Tissue Donation and Transplantation Authority: Agency Resources and Planned Performance, Department of Health and Ageing, 2013, Canberra, pp. 351 and 353.
118 Even with consent, some donations may not proceed for a variety of clinical reasons. The conversion rate is the proportion of cases where consent has been provided and donation proceeded.