Browse our range of reports and publications including performance and financial statement audit reports, assurance review reports, information reports and annual reports.
Auditor-General Report No. 31 of 2025–26
Effectiveness of the Commonwealth Home Support Program
Published
Thursday 14 May 2026

Portfolio
Health, Disability and Ageing
Entity
Department of Health, Disability and Ageing
Contact
Please direct enquiries through our contact page.
Activity
Service delivery
Sector
Health
Ageing
Audit snapshot
Why did we do this audit?
- Since 2015, the Commonwealth Home Support Program (CHSP) has provided entry‑level aged care services to people in their homes to assist them to live safely and independently. The Australian Government funds CHSP service providers through grant agreements.
- The Department of Health, Disability and Ageing (DHDA) is responsible for administering the CHSP.
- In response to recommendations of the 2021 Royal Commission into Aged Care Quality and Safety, the CHSP will transition to a new Support at Home program no earlier than 1 July 2027.
Key facts
- In 2024–25, the Australian Government provided $3.1 billion in CHSP grants to 1,273 providers. The CHSP is one of the Australian Government’s largest grant programs.
- In 2024–25, 838,694 people received CHSP services. Of these, DHDA estimated, based on a survey of providers, that approximately 113,000 people had not been assessed for aged care.
What did we find?
- The CHSP is partly effective. The CHSP is delivering services to more than 800,000 older people and an ANAO survey indicates that the majority of clients are satisfied. Weaknesses in administration of the program reduce effectiveness. DHDA lacks assurance that CHSP services are being delivered effectively, to eligible people, according to need, and in a timely manner.
- A lack of monitoring, assurance, evaluation and stakeholder engagement limits DHDA’s ability to identify and implement improvements to the program.
- Poor assurance over the current CHSP impacts on preparedness for the effective transition of the CHSP to the Support at Home program.
What did we recommend?
- There were nine recommendations to DHDA to improve planning, monitoring, stakeholder engagement, assurance, performance measurement and evaluation.
- DHDA agreed to all recommendations.
51%
The percentage of CHSP clients who believe that it is difficult to ‘receive aged care services in your home when you need them’.
65%
The percentage of CHSP clients who are satisfied with their overall experience of CHSP services.
54%
The percentage of CHSP clients who believe the CHSP has improved their level of independence.
This audit report is presented in two parts:
- Part A — Report at a glance
- Part B — Full report (this page)
Summary and recommendations
Background
1. The Commonwealth Home Support Program (CHSP) is an entry-level aged care program.1 The program has five objectives, which are to support older people who are having difficulties with daily living to: have a better quality of life; continue living in their own homes and/or delay admission to residential care; be able to participate more in their community and have more face-to-face and online social connections; maintain and/or improve their psychological, emotional and physical wellbeing; and be more independent at home and in the community.2 The Australian Government has provided $30.6 billion to fund CHSP services since the CHSP commenced in 2015–16. Funding is provided through grant agreements with CHSP service providers.
2. The Department of Health, Disability and Ageing (DHDA) is responsible for ‘services for older people, including their carers’.3 Its purpose includes to ‘support the Government to lead and shape Australia’s … aged care [system] … through evidence-based policy, well targeted programs, and best practice regulation’.4 DHDA manages the CHSP with the Department of Social Services through the Community Grants Hub and the Aged Care Quality and Safety Commission (ACQSC).
3. The 2021 Royal Commission into Aged Care Quality and Safety (Royal Commission) made 148 recommendations, including the establishment of a new aged care act and improved regulation, data, performance reporting and evaluation of aged care. Recommendation 25 was that, by 1 July 2024, the System Governor should implement a new aged care program that combines the CHSP with other in home aged care programs.5 The Aged Care Act 2024, originally scheduled for commencement on 1 July 2025, commenced on 1 November 2025. Changes included: from 1 November 2025, transition of the Home Care Packages Program and Short-Term Restorative Care Program to a new Support at Home program; from 1 November 2025, ACQSC registration and regulation of CHSP providers; and no earlier than 1 July 2027, transition of the CHSP to the Support at Home program.
Rationale for undertaking the audit
4. In 2024–25, the Australian Government provided $3.1 billion in funding to 1,273 CHSP providers, making it one of the Australian Government’s largest grants programs. In 2024–25 the CHSP accounted for eight per cent of the Australian Government’s total aged care expenditure of $38.87 billion. Almost 840,000 people used CHSP services in 2024–25. In anticipation of the transition of the CHSP to the Support at Home program no earlier than 1 July 2027, the audit provides assurance to Parliament on the extent to which DHDA has effectively delivered the CHSP and is achieving the program’s overarching objective to support older people to live safely and independently at home and in their communities.
Audit objective and criteria
5. The audit objective was to examine the effectiveness of the Commonwealth Home Support Program.
6. To form a conclusion against this objective, the ANAO adopted the following high-level criteria:
- Does the CHSP meet community need?
- Are CHSP services delivered effectively?
- Is the CHSP meeting its objectives?
Conclusion
7. The CHSP is delivering entry-level in home aged care services to more than 800,000 older people in Australia and ANAO survey data indicates that clients are largely satisfied with the services they receive. Despite being one of Australia’s largest grants programs, DHDA is unable to clearly demonstrate that the CHSP is meeting community demand or the program’s objectives. There are accessibility barriers to CHSP services and DHDA lacks assurance that CHSP services are being delivered effectively, to eligible people, according to need, and in a timely manner. The CHSP is partly effective due to these deficiencies in the administration of the program.
8. The CHSP is due to transition to the Support at Home program no earlier than 1 July 2027. DHDA will need to obtain more robust assurance over eligibility, unmet demand, provider sustainability, service delivery quality, and the achievement of objectives to effectively support the CHSP’s transition to the new program.
9. The CHSP is partly effective at meeting community need. While DHDA provides advice to government about supply and demand pressures to support additional funding, it does not have an established methodology for measuring and monitoring unmet demand for CHSP services. ANAO research has found that significant proportions of CHSP providers, peak bodies and CHSP clients perceive there to be accessibility barriers for CHSP services. In relation to readiness for transition to the Support at Home program from 1 July 2027, forecasting of both demand and supply is limited. Engagement with CHSP providers about demand pressures and supply constraints is limited. DHDA’s ability to determine if CHSP services are being provided to eligible people according to need in a timely manner is constrained by: controls that are still developing to ensure CHSP services are provided to those who have been assessed as needing them; system and data limitations that do not capture information about timeliness of service provision across the entire client journey; and a lack of monitoring.
10. An ANAO survey of more than 10,000 CHSP clients found that the majority were satisfied with their overall experience of CHSP services. DHDA’s assurance arrangements have focused on service provider reconciliation of grant funds based on provider self-reporting, not on the quality of service delivery, and are reactive. Stakeholder engagement does not fully support continuous improvement in service delivery, in part because there is little engagement with CHSP clients or about the client experience. There are oversight committee arrangements, but there is no program-level assurance framework for the CHSP and DHDA does not plan assurance activities to align with program risks. DHDA has not obtained appropriate assurance that CHSP services are delivered to people based on assessed need. DHDA obtains some information about service quality through delivery partners but does not have assurance over the quality of CHSP service delivery for the majority of providers. DHDA has not analysed complaints or identified lessons learnt from the CHSP to inform its transition to the Support at Home program.
11. DHDA has not demonstrated, through performance reporting or evaluation, that the CHSP is meeting its objectives (which comprise, for clients: better quality of life, delaying admission to residential aged care, greater social connectivity, improved or maintained emotional and physical wellbeing, and greater independence). There is a public performance measure for the CHSP that reports on outputs and provides no information about the achievement of outcomes or program efficiency. DHDA monitors some performance data that is primarily related to grant agreement financial acquittals and outputs. DHDA has not evaluated the CHSP and has commissioned little research that supports an understanding of impact. ANAO research has found that the majority of stakeholders (CHSP providers, peak bodies and CHSP clients) believe that most objectives are being met, particularly improved quality of life.
Supporting findings
Meeting community need
12. There is no robust planning framework for the CHSP. Effectiveness of arrangements to measure, monitor, plan for and advise on the demand for CHSP services is reduced by the absence of methodologies to calculate current demand or forecast future demand. A demand forecasting methodology is under development for the Support at Home program. Some work has been done on understanding and forecasting workforce trends, however DHDA has no documented methodology for forecasting the supplier market, either nationally or for specific geographic regions, cohorts or service types. DHDA monitors CHSP service provider overspends and underspends of grant funding, which provides some information about current demand and supply. Systems, data and tools available to monitor overspends and underspends are not fully utilised to understand all priority client groups. There is limited engagement with providers about demand and supply pressures. ANAO research and other evidence suggests there are demand and supply pressures on the CHSP. For example, 49 per cent of CHSP providers responding to an ANAO survey agreed or strongly agreed that ‘CHSP meets my community’s demand for services’, while 38 per cent disagreed or strongly disagreed; and 51 per cent of CHSP clients said that there was a time when they could not get an aged care service in their home or community that they needed, with the main barriers being ‘local providers of that service were not available’ and ‘local provider not accepting new clients’. (See paragraphs 2.8 to 2.40)
13. Upon commencement of the Aged Care Act 2024 on 1 November 2025, CHSP services were being provided to over 100,000 clients without a clear understanding of their needs as they have never been assessed for aged care services. This is not consistent with requirements under the Aged Care Act 2024 — a risk that DHDA is managing. Analysis of all aged care assessments shows that time elapsed between applying for an aged care assessment and completing the assessment increased from 12 days in 2017–18 to 27 days in 2024–25 at the 50th percentile. At the 90th percentile, the number of days increased from 67 to 172. For CHSP clients specifically, the elapsed time between referral to an assessment organisation and a completed assessment in 2024–25 was 21 days at the 50th percentile and 103 days at the 90th percentile. DHDA does not monitor the timeliness of the complete journey from assessment through to receipt of services from CHSP providers, due in part to system and data limitations. DHDA has some data that allows it to monitor time elapsed between a CHSP provider accepting a referral and providing a service but does not regularly analyse or monitor this. DHDA has not established timeliness benchmarks or targets for CHSP service delivery. Forty-two per cent of CHSP clients surveyed by the ANAO did not consider waiting times to receive aged care services in their home to be reasonable, and 51 per cent stated that it was somewhat or very difficult to ‘receive aged care services in your home when you need them’. (See paragraphs 2.42 to 2.57)
Delivering services effectively
14. DHDA has not established a CHSP stakeholder engagement plan to support meaningful engagement with people and communities to develop a fit-for-purpose program. DHDA provided three updates on the CHSP to older people, their families and carers between November 2022 and June 2025. Stakeholder engagement activities for the CHSP have focused on CHSP providers, and there has been limited to no focus on higher levels of stakeholder engagement (involvement, collaboration and empowerment) with any stakeholder groups. In ANAO surveys of CHSP providers and peak bodies, 37 per cent of providers agreed or strongly agreed DHDA had sought feedback on how the CHSP could be improved; and one of nine peak bodies agreed DHDA has engaged with CHSP clients, carers and representatives on their views of the effectiveness of CHSP service delivery. This is not consistent with the DHDA’s aged care engagement principles. Stakeholder engagement practices do not fully support DHDA to understand or improve the quality of CHSP service delivery. (See paragraphs 3.5 to 3.16)
15. While the Aged Care Quality and Safety Commission (ACQSC) and the Department of Social Services (DSS) have assurance responsibilities over CHSP service delivery quality, DHDA maintains responsibility for overall program delivery and effectiveness. DHDA has a committee structure to oversee the CHSP and has set out delivery partner roles and responsibilities through memoranda of understanding or similar. DHDA has a planning methodology for program assurance activities, which are intended to give decision-makers confidence that work is progressing as planned and in accordance with legal and policy frameworks. DHDA has not established a risk-based CHSP program-level assurance framework to support assurance planning for the CHSP and has not planned assurance activity in alignment with risk. CHSP projects that have been assessed as ‘tier 1’ (of significant importance to DHDA with a high level of risk, effort and investment to deliver) also do not have assurance plans. This is not consistent with DHDA’s Project Management Framework. (See paragraphs 3.18 to 3.31)
16. DHDA’s assurance activities for the CHSP have focused on assuring provider expenditure against allocated grants funding, which is based on provider self-reporting. DHDA acts on providers’ financial performance to improve program integrity. DHDA has not obtained full assurance that the right CHSP services are being delivered to people who need them. DHDA receives ACQSC and Community Grants Hub referrals of providers who are non-compliant with quality requirements. DHDA did not cancel any CHSP provider agreements based on the ACQSC’s assessment of non-compliance with the Aged Care Quality Standards in 2023–24 and 2024–25. DHDA has not obtained assurance over the overall quality of CHSP service delivery by the majority of CHSP providers. In an ANAO survey of CHSP providers, 87 per cent agreed or strongly agreed that CHSP services are of high quality. In an ANAO survey of CHSP clients, 65 per cent were satisfied or very satisfied with their overall experience of the services they received in the last six months. There is no analysis of complaints or compilation of lessons learnt to support the transition to the Support at Home program. (See paragraphs 3.33 to 3.55)
Is the Commonwealth Home Support Program meeting its objectives?
17. There is a lack of performance measurement, monitoring and reporting of program quality, outcomes or efficiency. DHDA has one corporate plan performance measure for the CHSP that measures output (number of clients that access CHSP services). DHDA reported that it ‘substantially met’ the measure’s target of 840,000 CHSP clients in 2024–25. DHDA has established provider performance measures that relate to provider financial compliance with grant agreements. DHDA monitors the corporate plan performance measure, provider financial compliance and other program statistics on a monthly basis. (See paragraphs 4.4 to 4.16)
18. Other than planning for an evaluation of one CHSP project, DHDA has not planned to evaluate the CHSP against its objectives and has not evaluated the appropriateness of CHSP funding arrangements and key policy settings. DHDA has conducted or commissioned reviews of some components of the CHSP. DHDA cannot demonstrate the CHSP is meeting the program’s objectives. (See paragraphs 4.17 to 4.27)
19. There is little available research that examines the impact of the CHSP or the extent to which the CHSP’s objectives are being met. Available data on the impact of in home aged care services more generally indicates a downward trend in the use of residential aged care (a CHSP objective), however there is a lack of longitudinal data that would help establish causality. ANAO research suggests that a majority of stakeholders (CHSP clients, aged care peak bodies and CHSP providers) believe that most objectives are being met. The proportion of CHSP clients that reported a little or a lot of improvement in outcomes ranged from 32 per cent (ability to participate in your community) to 66 per cent (quality of life). First Nations clients were less likely than average to report improved outcomes. (See paragraphs 4.28 to 4.29)
Recommendations
Recommendation no. 1
Paragraph 2.39
The Department of Health, Disability and Ageing implement appropriate measurement and monitoring of demand and supply pressures to support advice, decision-making, and planning for the Commonwealth Home Support Program, including as it transitions to the Support at Home program.
Department of Health, Disability and Ageing response: Agreed
Recommendation no. 2
Paragraph 2.45
The Department of Health, Disability and Ageing ensure compliance with the Aged Care Act 2024 by accurately quantifying the total number of unregistered clients, establishing a plan to ensure all Commonwealth Home Support Program clients have an aged care assessment, and setting a date for when this work is to be completed.
Department of Health, Disability and Ageing response: Agreed
Recommendation no. 3
Paragraph 2.58
To help determine whether Commonwealth Home Support Program services are being provided to people when they are needed and to inform program planning for the Support at Home program, the Department of Health, Disability and Ageing establish monitoring arrangements and benchmarks that allow it to assess and report on the timeliness of Commonwealth Home Support Program service delivery across the entire journey from first contact to service receipt.
Department of Health, Disability and Ageing response: Agreed
Recommendation no. 4
Paragraph 3.16
The Department of Health, Disability and Ageing develop a stakeholder engagement plan for the Commonwealth Home Support Program that:
- identifies stakeholders, engagement objectives and methods;
- considers approaches to ensure successful engagement with diverse audiences;
- includes direct engagement with participants, their families and carers;
- considers higher levels of engagement (involve, collaborate and empower);
- incorporates ongoing review and evaluation of engagement activities; and
- includes the transition to the Support at Home program.
Department of Health, Disability and Ageing response: Agreed
Recommendation no. 5
Paragraph 3.27
The Department of Health, Disability and Ageing establish a risk-based Commonwealth Home Support Program assurance framework to support the monitoring of quality service delivery and continuous improvement, including as the Commonwealth Home Support Program transitions to the Support at Home program.
Department of Health, Disability and Ageing response: Agreed
Recommendation no. 6
Paragraph 3.43
The Department of Health, Disability and Ageing work with the Aged Care Quality and Safety Commission and Department of Social Services to identify and respond to gaps in assigned assurance roles and responsibilities for the ongoing administration of the Commonwealth Home Support Program and its transition to Support at Home.
Department of Health, Disability and Ageing response: Agreed
Recommendation no. 7
Paragraph 3.50
The Department of Health, Disability and Ageing undertake risk-based assurance activities that provide confidence to decision makers that the Commonwealth Home Support Program is being managed within expectations and in accordance with legal and policy frameworks, including in relation to service delivery quality.
Department of Health, Disability and Ageing response: Agreed
Recommendation no. 8
Paragraph 4.11
The Department of Health, Disability and Ageing establish performance measures for the Commonwealth Home Support Program that facilitate monitoring of service delivery and public transparency over whether the program is efficiently meeting its objectives.
Department of Health, Disability and Ageing response: Agreed
Recommendation no. 9
Paragraph 4.30
The Department of Health, Disability and Ageing establish an evaluation plan for the Commonwealth Home Support Program and evaluate the extent to which the Commonwealth Home Support Program objectives are being met, to inform the Commonwealth Home Support Program’s transition to the Support at Home program.
Department of Health, Disability and Ageing response: Agreed
Summary of entity response
20. The proposed final report was provided to DHDA. The summary response from DHDA to the report is provided below. The full response is at Appendix 1.
The Department of Health, Disability and Ageing notes the findings of the report and agrees with all nine recommendations.
The department acknowledges the ANAO research finding that the majority of stakeholders (CHSP providers, peak bodies and CHSP clients) believe that most objectives are being met, particularly improved quality of life.
Following the introduction of the Aged Care Act 2024, the department is strengthening data collection arrangements to improve oversight of the program. Further work will be undertaken to better model program supply and demand pressures, including to inform future policy and operational decisions.
The department manages program assurance through strong and collaborative relationships with the Aged Care Quality and Safety Commission and the Department of Social Services. These arrangements will continue to be strengthened to support effective program delivery.
The CHSP will transition to Support at Home no earlier than July 2027, with future arrangements subject to decisions of Government. The department’s implementation of the recommendations from this report will reflect any decisions of government regarding the future direction and management of the CHSP.
Key messages from this audit for all Australian Government entities
21. Below is a summary of key messages, including instances of good practice, which have been identified in this audit and may be relevant for the operations of other Australian Government entities.
In designing and implementing large-scale grant programs to meet community needs, Australian Government entities should take into account the following key messages from this audit.
- The need for good planning applies equally to ‘legacy’ and long-running programs as it does to new programs — Sound planning is based on high-quality data and analysis to ensure services remain responsive to the diverse needs of people. A good understanding of demand pressures and supply constraints supports effective and efficient program delivery, fit for purpose policy advice and security of future services. Robust forecasting methodologies are particularly important in sectors where there is significant demographic and structural change.
- The design and ongoing administration of programs will benefit from meaningful stakeholder engagement — One of four ‘pillars’ of the Australian Public Service (APS) Reform program is that ‘the APS puts people and business at the centre of policy and services’. High quality engagement with external stakeholders, and especially service recipients, supports entities to advise on, design, develop and deliver more effective programs and services. The Australian Government’s Charter of Partnerships and Engagement provides principles for stakeholder engagement in the APS, and includes better practice tools and resources for how to lift the quality of engagement from simply ‘sharing information’ to ‘collaborating’ and ‘empowering’.
- Where services are delivered through market-based providers, Australian Government entities retain responsibility for assuring quality delivery — Quality service delivery not only benefits service recipients, it ensures that value for money is being achieved for all Australian taxpayers. Appropriate assurance over program delivery provides confidence to leaders and decision makers that activities are being managed within expectations and in accordance with legal and policy frameworks. Appropriate assurance is particularly important where programs have higher budgets, complexity, risk or impact. The starting point for effective assurance is an assurance framework that sets out existing and planned assurance activities mapped to risk. Where multiple entities are involved in assurance, roles and responsibilities should be clear. Entities should establish suitable measures of performance and evaluation plans to demonstrate program effectiveness and efficiency.
1. Background
Introduction
1.1 Australia’s aged care system provides subsidised care and support to older people through services ranging from basic support to people in their homes to comprehensive 24-hour care in residential care homes. To access aged care services, a person normally undergoes an assessment to determine the level of care and support they may be eligible for, with different aged care programs having different eligibility criteria.6
1.2 The Department of Health, Disability and Ageing (DHDA) is responsible for ‘services for older people, including their carers’.7 Its purpose includes to ‘support the Government to lead and shape Australia’s … aged care [system] … through evidence-based policy, well targeted programs, and best practice regulation’.8 Under the Aged Care Act 2024, the Secretary of DHDA is the aged care ‘System Governor’, whose role includes: facilitating equitable access to aged care services; providing stewardship of the administration of aged care; and protecting and upholding the integrity of the administration of the aged care system and the Commonwealth’s investment in the system.9
Commonwealth Home Support Program
1.3 The Commonwealth Home Support Program (CHSP) is an entry-level aged care program intended to support older people to live independently in their homes and communities.10 Two other in home aged care programs — the Home Care Packages Program11 and Short-Term Restorative Care Program12 — catered to higher support needs prior to transitioning to the Support at Home program on 1 November 2025 (see paragraph 1.14).
1.4 The CHSP was established on 1 July 201513 (see Appendix 3) and has five objectives, which are to support older people who are having difficulties with daily living to:
- have a better quality of life;
- continue living in their own homes, and/or delay admission to residential care;
- be able to participate more in their community and have more face-to-face and online social connections;
- maintain and/or improve their psychological, emotional and physical wellbeing; and
- be more independent at home and in the community.14
1.5 The CHSP has three aims:
- to help older people live as independently as possible;
- to focus on working with them, rather than doing things for them; and
- to give a small amount of help to a large number of people.15
1.6 In 2025–26 service types provided through the CHSP comprised:
- home support (allied health and therapy services, domestic assistance, hoarding and squalor assistance, home maintenance and repairs, meals, personal care, nursing care, community cottage respite, home or community general respite, social support and community engagement, therapeutic services for independent living, and transport);
- home modifications (home adjustments);
- assistive technology (equipment and products);
- advisory services (specialised support services); and
- sector support and development.16
1.7 DHDA advised the ANAO in April 2026 that state and territory funded service providers were transitioned to the CHSP when it commenced in 2015 and until 30 June 2018 through a direct sourcing arrangement approved by the Minister for Health. From 1 July 2018, the Australian Government funded CHSP services through grant agreements (see Appendix 3 for a timeline of CHSP extensions). Ad hoc17, demand driven18, closed non-competitive and targeted competitive grants19 were used to provide funding for trialling and implementing new service delivery models, expanding coverage in targeted regions and for certain service types, and replacing providers that ceased service delivery. Grant funds are allocated for individual service types with flexibility provisions that allow providers to re-allocate some grant funding between service types, depending on demand in their communities.
1.8 The CHSP is a capped rather than demand-driven program, with total funding budgeted to the program determined by government. In 2024–25, 838,694 people received CHSP services from 1,273 providers. Between 2015–16 and 2024–25, expenditure on the CHSP increased from $2.2 billion to $3.3 billion. In real dollars (Figure 1.1), CHSP expenditure peaked in 2021–22. In the same period, Australian Government expenditure on the broader aged care portfolio increased in real dollars. In 2024–25, DHDA’s annual report stated that CHSP grants totalled $3.1 billion.20
Figure 1.1: Australian Government aged care expenditurea, adjusted to real dollar valuesb, 2015–16 to 2024–25
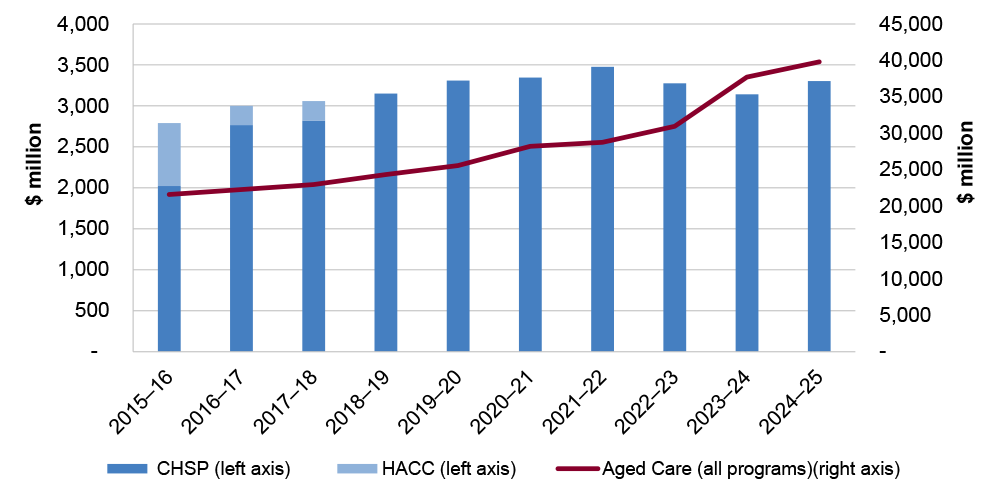
Note a: In Victoria and Western Australia, Commonwealth Home and Community Care (HACC) clients transitioned to the CHSP on 1 July 2016 and 1 July 2018, respectively.
Note b: Time series financial data is adjusted using the Australian Bureau of Statistics general government final consumption expenditure (GGFCE) deflator so that comparisons are based on real dollar amounts that reflect actual purchasing power. Values are expressed in terms of 2024–25 dollars.
Source: ANAO analysis of Productivity Commission, Report on Government Services 2025, Part F, Section 14, Aged care services — data tables, Table 14A.6 and Productivity Commission, Report on Government Services 2026, 2, Statistical Context, PC, 2026, available from https://www.pc.gov.au/ongoing/report-on-government-services/approach/statistical-context/ [accessed 15 April 2026].
1.9 To be eligible for the CHSP, people must undergo an aged care assessment to determine their support needs and, as at 1 November 2025, be aged: 65 years or older; 50 years or older for Aboriginal or Torres Strait Islander person; or 50 years or older and be homeless or at risk of homelessness.21
1.10 DHDA is responsible for administering the CHSP.22 The Community Grants Hub within the Department of Social Services administers CHSP grant agreements with providers on behalf of DHDA. The Aged Care Quality and Safety Commission is the national regulator of aged care services and works with DHDA on matters relating to provider compliance with the Aged Care Quality Standards.2324
1.11 Figure 1.2 sets out the client journey through the aged care system, the relationship between the CHSP and other aged care programs administered by DHDA, and other Australian Government agencies with responsibilities in aged care.
Figure 1.2: Client journey through the aged care system
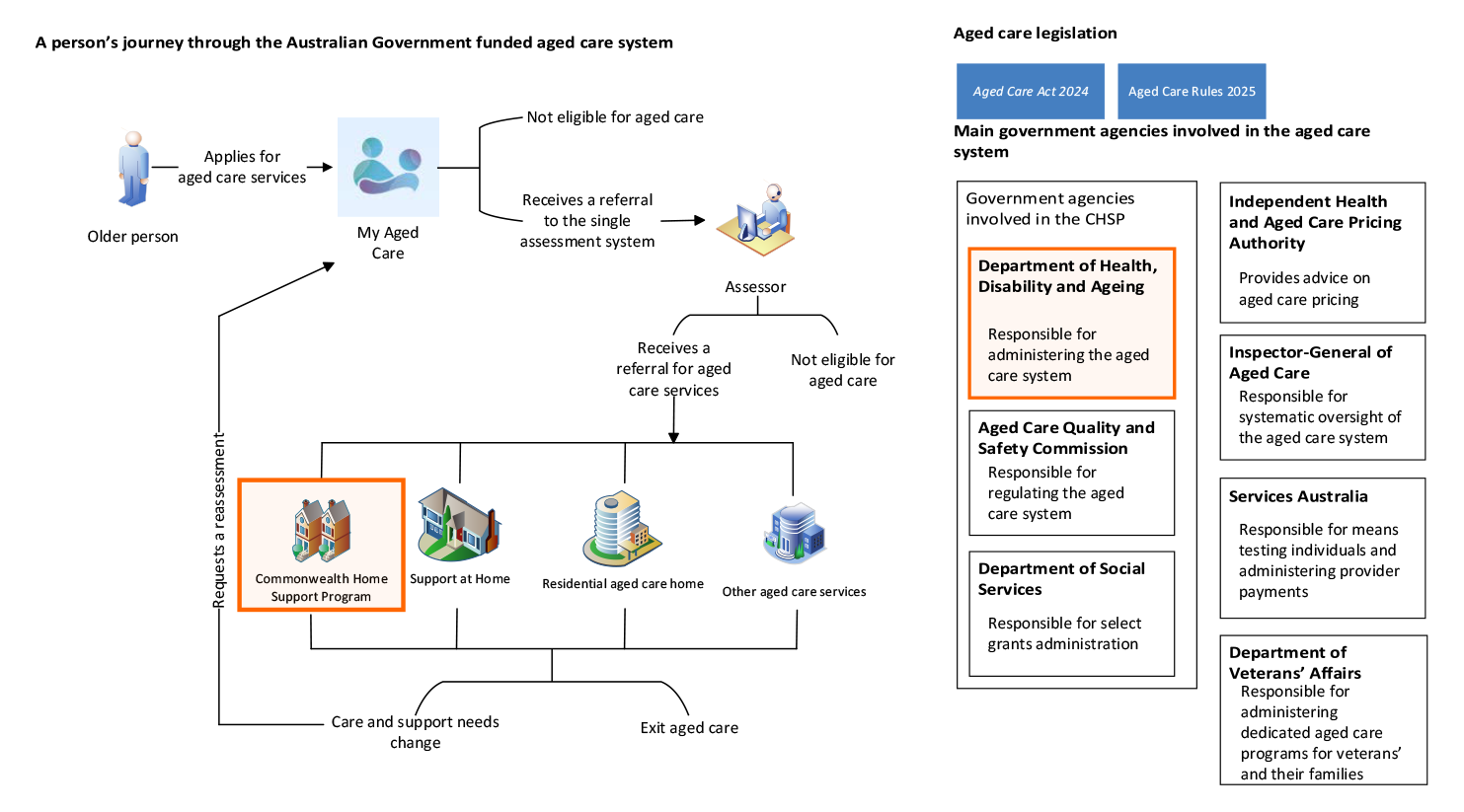
Source: ANAO analysis.
Aged care reforms
1.12 The Royal Commission into Aged Care Quality and Safety (Royal Commission) report tabled in the Parliament on 1 March 2021. The report stated that:
Most older people want to remain living in their own homes, rather than moving to residential aged care. However, in the current aged care system, older people often wait too long to get access to care at home … may receive less care than they need, or they may not have access to specific services they need. Without access to home care services that meet their assessed needs, people face risks of declining function, preventable hospitalisation, carer burnout, premature entry to residential aged care, and even death.25
1.13 The Royal Commission made 148 recommendations including the establishment of a new aged care act and improved regulation, data, performance reporting and evaluation of aged care.26 Four recommendations directly related to the CHSP (Box 1).
|
Box 1: Royal Commission recommendations relating to the Commonwealth Home Support Program |
|
1.14 The Australian Government responded to Royal Commission recommendations through the 2021–22 Federal Budget measure Home Care – Future design and funding, which included funding for the development of a new Support at Home program.27 The Aged Care Act 2024, originally scheduled for commencement on 1 July 2025, commenced on 1 November 2025, replacing the Aged Care Act 1997; Aged Care (Transitional Provisions) Act 1997; and Aged Care Quality and Safety Commission Act 2018. The new Act established a new regulatory model and made other changes including:
- from 1 July 2024, phased introduction of a single assessment system to determine eligibility for aged care services, replacing three assessment arrangements;
- from 1 November 2025, transition of the Home Care Packages Program and Short-Term Restorative Care Program to the new Support at Home program;
- from 1 November 2025, Aged Care Quality and Safety Commission registration and regulation of CHSP providers; and
- no earlier than 1 July 2027, transition of the CHSP to the Support at Home program.28
1.15 CHSP payments are generally made through a monthly grant payment in arrears.29 Under the Support at Home program, CHSP providers will be required to invoice the Australian Government based on services provided (a fee-for-service model).
Rationale for undertaking the audit
1.16 In 2024–25, the Australian Government provided $3.1 billion in funding to 1,273 CHSP providers, making it one of the Australian Government’s largest grants programs. In 2024–25 the CHSP accounted for eight per cent of the Australian Government’s total aged care expenditure of $38.87 billion. Almost 840,000 people used CHSP services in 2024–25. In anticipation of the transition of the CHSP to the Support at Home program no earlier than 1 July 2027, the audit provides assurance to Parliament on the extent to which DHDA has effectively delivered the CHSP and is achieving the program’s overarching objective to support older people to live safely and independently at home and in their communities.
Audit approach
Audit objective, criteria and scope
1.17 The audit objective was to examine the effectiveness of the Commonwealth Home Support Program.
1.18 To form a conclusion against this objective, the following high-level criteria were adopted:
- Does the CHSP meet community need?
- Are CHSP services delivered effectively?
- Is the CHSP meeting its objectives?
1.19 The audit did not examine the awarding of grant funding to CHSP providers; regulation by the Aged Care Quality and Safety Commission; or the Community Grants Hub’s administration of CHSP grants, including the collection or maintenance of CHSP data.
Audit methodology
The audit report is presented in two parts:
- Part A — Report at a glance; and
- Part B — Full report (this part).
Part A has been prepared to improve the accessibility of the full report, and includes what the audit examined, what was concluded, and key audit findings.
1.20 The audit involved:
- examination of DHDA’s records;
- meetings with DHDA officials;
- analysis of CHSP performance, CHSP expenditure and aged care assessment data;
- analysis of 59 contributions to the audit received from CHSP providers, clients and aged care peak bodies;
- meetings with aged care peak bodies representing CHSP providers and older people;
- collection and analysis of data from surveys of 495 employees of 436 CHSP provider organisations (see Appendix 4), nine aged care peak bodies (see Appendix 5) and 10,125 CHSP clients (see Appendix 6).
1.21 The ANAO acknowledges and thanks those who provided input into the performance audit through participation in ANAO surveys or making a submission to the audit — including CHSP clients, their carers, CHSP providers, aged care peak bodies and older persons’ advocacy organisations.
1.22 Australian Government entities largely give the ANAO electronic access to records by consent, in a form useful for audit purposes. For the purposes of this audit, DHDA advised the ANAO that it would not voluntarily provide certain information requested by the ANAO due to concerns about its obligations under the Privacy Act 1988 and the Public Interest Disclosure Act 2013 as well as the secrecy provisions in Health and Aged Care portfolio legislation. DHDA advised that this type of information largely was not segregated in the department’s records management systems and it could not be certain, in providing documents through electronic means, that documents containing this type of information were excluded. On 6 May 2025, the Auditor-General issued the Secretary of DHDA with a notice directing the Secretary to provide information and produce documents pursuant to section 32 of the Auditor-General Act 1997. Under this notice, DHDA provided the information and documents requested through electronic means.
1.23 The audit was conducted in accordance with ANAO Auditing Standards at a cost to the ANAO of approximately $905,000.
1.24 The team members for this audit were Michael Commens, Rebecca Storen, Lily Engelbrethsen, Benjamin Foreman, Joanna Giang and Christine Chalmers.
2. Meeting community need
Areas examined
This chapter examines whether the Commonwealth Home Support Program (CHSP), administered by the Department of Health, Disability and Ageing (DHDA) meets community need.
Conclusion
The CHSP is partly effective at meeting community need. While DHDA provides advice to government about supply and demand pressures to support additional funding, it does not have an established methodology for measuring and monitoring unmet demand for CHSP services. ANAO research has found that significant proportions of CHSP providers, peak bodies and CHSP clients perceive there to be accessibility barriers for CHSP services. In relation to readiness for transition to the Support at Home program from 1 July 2027, forecasting of both demand and supply is limited. Engagement with CHSP providers about demand pressures and supply constraints is limited. DHDA’s ability to determine if CHSP services are being provided to eligible people according to need in a timely manner is constrained by: controls that are still developing to ensure CHSP services are provided to those who have been assessed as needing them; system and data limitations that do not capture information about timeliness of service provision across the entire client journey; and a lack of monitoring.
Areas for improvement
The ANAO made three recommendations for DHDA to improve measurement and monitoring of demand and supply pressures; establish a plan and timeframe for ensuring CHSP clients are registered and assessed; and establish arrangements to monitor timeliness of CHSP service provision.
2.1 The object of the Aged Care Act 2024 includes:
- providing a forward-looking aged care system that is designed to assist individuals accessing funded aged care services to live active, self-determined and meaningful lives; and
- ensuring equitable access to, and flexible delivery of, funded aged care services that put older people first and take into account the needs of individuals, regardless of their location, background and life experience.30
2.2 The Commonwealth Home Support Program — Program Manual 2025–27 (November 2025) (CHSP Manual) states that certain groups may require tailored support according to their needs, including people from culturally and linguistically diverse backgrounds; people who identify as Aboriginal and/or Torres Strait Islander; or people who live in rural and remote areas of Australia.31
2.3 The function of policy advice is to provide decision-makers with the information they need to make the best possible decision. The Australian Public Service Commission’s Delivering Great Policy guidance states that policy advice should be informed by evidence, including stakeholder feedback and lessons from experience, and should consider the wider context for the policy, now and into the future.32
Are there effective arrangements to monitor and plan for demand and supply of services?
There is no robust planning framework for the CHSP. Effectiveness of arrangements to measure, monitor, plan for and advise on the demand for CHSP services is reduced by the absence of methodologies to calculate current demand or forecast future demand. A demand forecasting methodology is under development for the Support at Home program. Some work has been done on understanding and forecasting workforce trends, however DHDA has no documented methodology for forecasting the supplier market, either nationally or for specific geographic regions, cohorts or service types. DHDA monitors CHSP service provider overspends and underspends of grant funding, which provides some information about current demand and supply. Systems, data and tools available to monitor overspends and underspends are not fully utilised to understand all priority client groups. There is limited engagement with providers about demand and supply pressures. ANAO research and other evidence suggests there are demand and supply pressures on the CHSP. For example, 49 per cent of CHSP providers responding to an ANAO survey agreed or strongly agreed that ‘CHSP meets my community’s demand for services’, while 38 per cent disagreed or strongly disagreed; and 51 per cent of CHSP clients said that there was a time when they could not get an aged care service in their home or community that they needed, with the main barriers being ‘local providers of that service were not available’ and ‘local provider not accepting new clients’.
Planning and advice to government on program demand and supply
2.4 The CHSP Manual 2025–27 references a CHSP ‘Planning Framework’33, which it describes as an approach to plan for funding and ongoing program management based on the Aged Care Planning Regions, to ‘ensure the requirements of clients are considered, and funding is allocated so that growth in CHSP complements and enhances services already being delivered.’34 The CHSP Manual states that the CHSP Planning Framework requires consideration in planning of: existing services available in a given region, aged care approvals, projected growth in the target population and other factors influencing service delivery supply and demand; and parallel planning cycles, and processes in other related sectors, including broader aged care needs and the disability care sector.
2.5 Previous versions of the CHSP manual included an internal link to the CHSP Planning Framework, which no longer functions. DHDA advised the ANAO in August 2025 that there is no separate Planning Framework document beyond the brief and high-level description in the CHSP Manual 2025–27. There are no documented procedures to determine a planning cycle; identify data and intelligence sources to inform planning; nor set out methodologies for determining and forecasting need, demand, market constraints, supplier capacity and workforce for the CHSP. DHDA has not established tools for implementing and documenting the application of the CHSP Planning Framework.
2.6 Between 1 July 2023 and 30 June 2025, DHDA advised government to fund CHSP ‘growth rounds’ and agree to other initiatives. Some of this advice referred to demand, excess demand, supplier capacity and service continuity issues (Table 2.1).
Table 2.1: Advice to government on Commonwealth Home Support Program supply and demand pressures, July 2023 to June 2025
|
Date of advice |
Description of advice |
|
October 2023 |
Advice to the Minister for Aged Care (the Minister) regarding an ad hoc grant opportunity states that ‘in lieu of full open competitive grant rounds, this grant opportunity is the only available mechanism available for existing CHSP providers to address excess demand for services and acts principally as a release valve for major demand pressure facing CHSP’. |
|
December 2023 |
DHDA advised government on a 2024–25 First Nations growth funding grant opportunity, stating that the grant would increase the availability of culturally safe CHSP services and provide an entry pathway for Aboriginal Community Controlled Organisations (ACCOs) to enter the aged care market where they deliver across the care and support economy. The Minister agreed to a $10 million grant opportunity to provide additional funding to ACCOs with existing infrastructure that were able to rapidly deploy resources where there was excess demand. On 13 August 2024 the DHDA delegate approved $10 million in growth grants to 19 Indigenous CHSP providers. |
|
The Minister agreed to a $100 million growth grant funding round to be undertaken to address excess demand for certain service types (see paragraph 2.7), using a targeted competitive grants process open to existing and new CHSP providers. Advice to the Minister stated that these service types were identified through quantitative and qualitative measures of demand pressures. On 13 September 2024 the DHDA delegate approved $100 million in grants to 41 existing and 98 new CHSP providers. |
|
|
March 2024 |
The government agreed to a proposal to recover and re-allocate unspent and uncommitted CHSP funds with the aim of providing services to an additional 5,000 people not receiving CHSP services. |
|
October 2024 |
DHDA advised the government on the increasing trend of local government CHSP providers exiting the CHSP, stating that there were 148 local government providers funded to deliver CHSP services in 2024–25, a 30 per cent decrease from 214 providers in 2018–19. |
|
DHDA advised the government on a grant opportunity intended to fund CHSP providers to increase wages for home care employees.a Advice stated that the proposed grant opportunity would support CHSP providers to meet their legal obligations and maintain safe, quality care to the growing number of older Australians accessing CHSP services. The Minister agreed to a spending proposal of up to $17.1 million for this purpose. |
|
|
November 2024 |
DHDA advised the Minister that it was analysing CHSP demand for an intended 2025–26 growth funding round. |
|
December 2024 |
The Minister agreed to several proposals including a closed non-competitive grant extension round for existing CHSP providers, valued at $7.2 billion for two years until 30 June 2027, with the option to extend agreements for another one or two years. The advice stated that the proposals would ensure continuity for providers and clients as CHSP transitioned to operating under the new Aged Care Act 2024 by 1 July 2025 and to the Support at Home program by no earlier than 1 July 2027. |
|
February 2025 |
DHDA provided the Minister with five spending proposals to reallocate unspent CHSP funds, three of which were agreed. Agreed proposals comprised an emergency and critical needs grant opportunity ($15 million over three years from 2024–25); an increase in funding for the GEAT2GO sub-programb ($7 million in 2024–25 and $50 million in 2025–26); and Independent Living Assessment funding ($10.6 million over two years from 2025–26).c The Minister did not agree to a proposed $120 million growth funding opportunity for 2025–26 and 2026–27 nor a $30 million spending proposal for sector support and development in 2026–27. DHDA advised the Minister that if these proposals were not supported, excess demand for CHSP services would increase, which would result in additional pressures on the Support at Home program. DHDA advised the ANAO in September 2025 that the work was paused pending government consideration of the interface between CHSP and the Home Care Packages Program in the context of the implementation of the Aged Care Act 2024. |
|
May 2025 |
In an incoming government brief, the Minister was advised that external and internal readiness to implement the Aged Care Act 2024 on 1 July 2025 was being closely monitored with some providers raising concerns about their ability to meet intended transition timeframes, as well as issues with the implementation of IT systems changes. |
|
On 28 May 2025, DHDA advised the Minister for Aged Care and the Minister for Health and Ageing of risks and issues relating to the implementation of the Aged Care Act 2024 on 1 July 2025, which for CHSP included that CHSP providers would not be able to provide services to unassessed clients (see paragraph 2.43). The advice also stated that current CHSP grant agreements with providers would cease on 30 June 2025 and that new agreements were being agreed with over 1,300 CHSP providers. The advice recommended delaying commencement of the new Act in part to preserve service continuity. The Ministers agreed to defer the commencement of the Act to 1 November 2025. |
|
Note a: On 17 September 2024, the government announced a commitment of $3.8 billion to support increased wages by between 2.3 per cent and 13.5 per cent for eligible aged care workers employed under the Aged Care Award 2010 or the Social, Community, Home Care and Disability Services Industry Award 2010.
Note b: GEAT2GO is a service supplying equipment and technology with the aim of maintaining or increasing independence for CHSP clients.
Note c: The Commonwealth contracts Independent Living Assessment to provide aged care assessments.
Source: ANAO analysis.
2.7 DHDA advised the ANAO in September 2025 that CHSP planning ‘is not scheduled’ and ‘occurs on a case-by-case basis associated with each CHSP growth funding round’. In December 2023 the Minister agreed to $100 million in growth funding (see Table 2.1) based on a method which applied some aspects of the CHSP Planning Framework, such as aged care assessment referrals and historical service usage for Aged Care Planning Regions, but did not consider parallel planning cycles and processes in other related sectors, including broader aged care needs and the disability care sector. There is no evidence of the CHSP Planning Framework being implemented as described in other planning activities or to inform other government advice. DHDA advised the ANAO in April 2026 that planning and timelines for transition of the CHSP to the Support at Home program are subject to decisions of government.
Monitoring demand and supply
Demand for the Commonwealth Home Support Program
2.8 The Australian Bureau of Statistics found that in 2022, 1.7 million older Australians required assistance with at least one personal or everyday task. The CHSP provided 31.8 million service sessions to 834,981 people in 2023–24, and 32.3 million service sessions to 838,694 people in 2024–25. Domestic assistance, meals, transport, and nursing accounted for more than half of all services provided through the CHSP. Between 2020–21 and 2024–25, the Older Persons Advocacy Network’s (OPAN) ‘presenting issues’ raised concerns with in home service availability and accessibility, particularly in rural and remote communities.35
2.9 The Department of Social Services (DSS) publishes annualised data on the number of people accessing aged care in a ‘Care Sector Demand Map’, which can be filtered by program type, Aboriginal and Torres Strait Islander client status and culturally and linguistically diverse (CALD) client status.36 The Australian Institute of Health and Welfare’s (AIHW) ‘GEN Aged Care Data’ website has national data on aged care providers, aged care spending, and people using aged care, which can be disaggregated by program, gender, age, Aboriginal and Torres Strait Islander status and CALD status37, and which includes a CHSP dashboard.38 DHDA refers to this public data.
2.10 DHDA produces a monthly ‘performance report’ and a Home Support Operations Branch (HSOB) ‘data dashboard’, each of which includes information about CHSP expenditure at the service type level. The HSOB data dashboard also includes the current number of people receiving CHSP services, disaggregated by Aboriginal and Torres Strait Islander and CALD status (total and by service type).
2.11 Excess demand is where the demand for a good or service exceeds the quantity of a good or service available in the market. DHDA does not have a methodology for calculating excess demand for CHSP services. The absence of a methodology impedes decision-makers’ understanding of unmet demand for the CHSP and DHDA’s ability to provide evidence-based advice about CHSP funding. For example, a December 2023 ministerial brief sought approval for an additional $100 million in CHSP ‘growth funding’ (see Table 2.1) for four service types (domestic assistance, home maintenance, allied health and transport). The brief stated that these service types had excess demand, determined through comparing client referrals at the Aged Care Planning Regions level39 using My Aged Care40 assessment outcomes and Aged Care Data Warehouse service delivery data41). The advice for growth funding was inconsistent with the results of the methodological approach as described, as the advice included growth funding for one service area (allied health and therapy) where the number of services exceeded the number of referrals. The described approach to calculating excess demand was not re-used in other analysis or advice between 1 July 2023 and 1 November 2025.
2.12 Ad hoc grants were made available to existing CHSP providers to address excess demand following a decision of government to extend the CHSP for an additional year from 1 July 2024 until 30 June 2025 (government later agreed to extend the CHSP until at least 30 June 2027). In addition to unforeseen and exceptional circumstances, delivery service sector improvements or new and innovative home-support delivery models, ad hoc grants were intended to respond to demonstrated service demand pressures and supply shortages. Applicants were required to fully address the assessment criteria (which were: proposal is consistent with the objectives of the CHSP, demonstrates organisational capacity and performance, and addresses implementation risks) and set out proposed costings and expected outputs. DHDA officials were responsible for assessing applications and determining the amount of funds allocated. There is no evidence that the award of funding for service demand pressures and supply shortages was based on a clear and consistent methodology for calculating excess demand.
2.13 In October 2025 the Senate Community Affairs References Committee published its report on aged care service delivery, which states:
The committee received overwhelming evidence that demand for CHSP services is currently far in excess of available funding, and that providers are forced to turn away clients seeking assistance.42
2.14 In November to December 2025, the ANAO invited 159,997 CHSP clients to provide feedback on CHSP services through an online survey (see Appendix 6). In total, 10,125 clients completed the survey (6.5 per cent response rate). Results from questions relating to demand for services are shown in Box 2 and demonstrate that for the majority of existing CHSP clients, access to CHSP and other in home aged care services was perceived to be difficult.
|
Box 2: ANAO surveys — demand for Commonwealth Home Support Program services |
|
In relation to current demand for CHSP services:
|
2.15 DHDA does not monitor excess demand. The HSOB data dashboard includes the year-to-date total number of recommendations and referrals for CHSP services at the national level and of active CHSP referrals at the time the dashboard is prepared. This information is not shown by service type43, and referrals are not directly compared to current service usage to arrive at a point-in-time excess demand estimate that would enable ongoing monitoring of excess demand at the national level or by service type. DHDA does not monitor wait times for CHSP service delivery or complaints (see paragraphs 2.49 and 2.53).
2.16 Regular ‘intelligence reports’ developed by DHDA, DSS and the Aged Care Quality and Safety Commission (ACQSC) from July 2023 contained content relating to demand for specific services and from specific groups. For example, intelligence reports stated that demand for culturally appropriate services was outstripping supply and highlighted high demand for several service types (home maintenance; allied health; nursing; goods, equipment, and assistive technology; domestic assistance; and meals) and lower demand for respite care. The reports discussed that some CHSP clients with higher needs were using CHSP services while waiting for a Home Care Package (see paragraph 1.3). DHDA does not have any procedures that set out how it will use this intelligence in planning and there was no evidence of DHDA using this intelligence in a systematic way to monitor or respond to excess demand. For example, the grant opportunity guidelines for a First Nations growth funding round stated that growth funding would target new Aboriginal Community Controlled Organisations (ACCOs), to increase the availability of culturally safe CHSP services where there is an unmet demand, and that applicants would need to demonstrate unmet demand for First Nations people in the aged care planning region they intended to provide services. DHDA did not refer to intelligence or analysis of unmet demand for First Nations peoples in its advice to government supporting the First Nations growth funding round.
Supplier market, workforce and capacity to deliver
2.17 Intelligence reports from July 2023 to May 2025 identified several risks and issues relevant to the CHSP supplier market and workforce (see paragraph 2.16). These included:
- providers relinquishing services, including a number of Victorian local councils;
- financial viability of providers amid inflation and rising costs;
- service gaps in remote communities;
- high costs and challenges meeting cultural obligations;
- widespread workforce shortages, especially in regional and remote areas;
- high staff turn-over and difficulty recruiting and retaining staff and volunteers;
- some Indigenous providers relinquishing services due to administrative burden; and
- language barriers impacting access to and understanding of the aged care assessment process and the CHSP, and shortage of bilingual staff to assist.
2.18 In September 2025, the ANAO invited 1,486 employees of 1,168 CHSP providers and 19 peak bodies to provide feedback on the effectiveness of CHSP services through an online survey (see Appendix 4 and Appendix 5). In total, 495 people from 436 provider organisations (33 per cent response rate) and representatives of nine peak bodies (47 per cent response rate) completed the surveys. Box 3 provides results from questions about supplier capacity and shows that a substantial proportion of providers and the majority of peak providers believed that CHSP demand is outstripping supply and that DHDA’s consultation with them on supply issues is inadequate.
|
Box 3: ANAO surveys — supply of Commonwealth Home Support Program services |
|
In relation to current supply of CHSP services:
In relation to consultation on current supply and supplier capacity for CHSP services:
|
Note a: Providers delivering services in the Australian Capital Territory (ACT) and South Australia (SA) were less likely than average to agree or strongly agree that ‘CHSP services are accessible to those who need them’ (41 and 42 per cent respectively) and providers from Tasmania were more likely than average to disagree (43 per cent).
2.19 In 2023 DHDA commissioned an Aged Care Provider Workforce Survey to obtain information on the size, composition and characteristics of the aged care workforce in residential and in home care settings.44
2.20 Other than the 2023 survey, DHDA monitoring of supplier capacity is primarily focused on current CHSP provider capacity to deliver services for which grants funding already has been awarded (underspend and overspend). The Data Exchange (DEX) system, managed by DSS, allows CHSP service providers to report service delivery information to the Community Grants Hub. Data from DEX is imported into the Aged Care Data Warehouse (see paragraph 2.11) every six months at DHDA’s request. The Aged Care Data Warehouse is the primary data used by DHDA for the purpose of monitoring and reporting against the corporate plan performance measure described in paragraph 2.30. DHDA uses real time Qlik Sense reports and IBM Cognos to support other types of analyses of Aged Care Data Warehouse holdings.45 The monthly performance reports and HSOB data dashboard (see paragraph 2.12) include information on funds allocated and expended at the program and service levels. DSS publishes annualised data on CHSP expenditure and the number of CHSP providers in the Care Sector Demand Map (see paragraph 2.9), at the level of postcode, local government area and other geographic criteria.46
2.21 For the CHSP, DHDA calculates underspend at the service type level by comparing expended grants funding to allocated grants funding. DHDA monitors underspend and overspend through the monthly performance report and HSOB data dashboard (see paragraph 2.10). The monthly performance reports show expenditure at a program level (nationally) and by service type and include explanatory narrative and trends. The HSOB data dashboards include point in time information on the number of providers and the ratio of CHSP funds expended to allocated for the whole of the CHSP and for each service type.
2.22 As shown in Table 2.1, in March 2024 DHDA advised government on a proposal to recover and re-allocate unspent and uncommitted CHSP funds with the aim of providing services to an additional 5,000 people not receiving CHSP services. DHDA also has processes for recovering and reallocating funds from some CHSP providers that are not fully utilising allocated funds to provide services (see paragraph 3.40).
2.23 Since the HSOB data dashboard was first produced in February 2024, the ratio of funds expended to allocated ranged from 78 to 86 per cent at the whole of program level. ANAO analysis of annual expenditure from 2021–22 to 2024–25 shows that for nine service types, the ratio was less than 100 per cent, indicating underspend (Figure 2.1). Total underspends across three years was greatest for respite care services. For 10 service types, the ratio was equal to or greater than 100 per cent, indicating allocated grants funds for those services were exhausted and that providers were using underspends in other service areas to meet client needs; this was greatest for domestic assistance.
Figure 2.1: CHSP underspend and overspenda,b by CHSP service type, 2021–22 to 2024–25
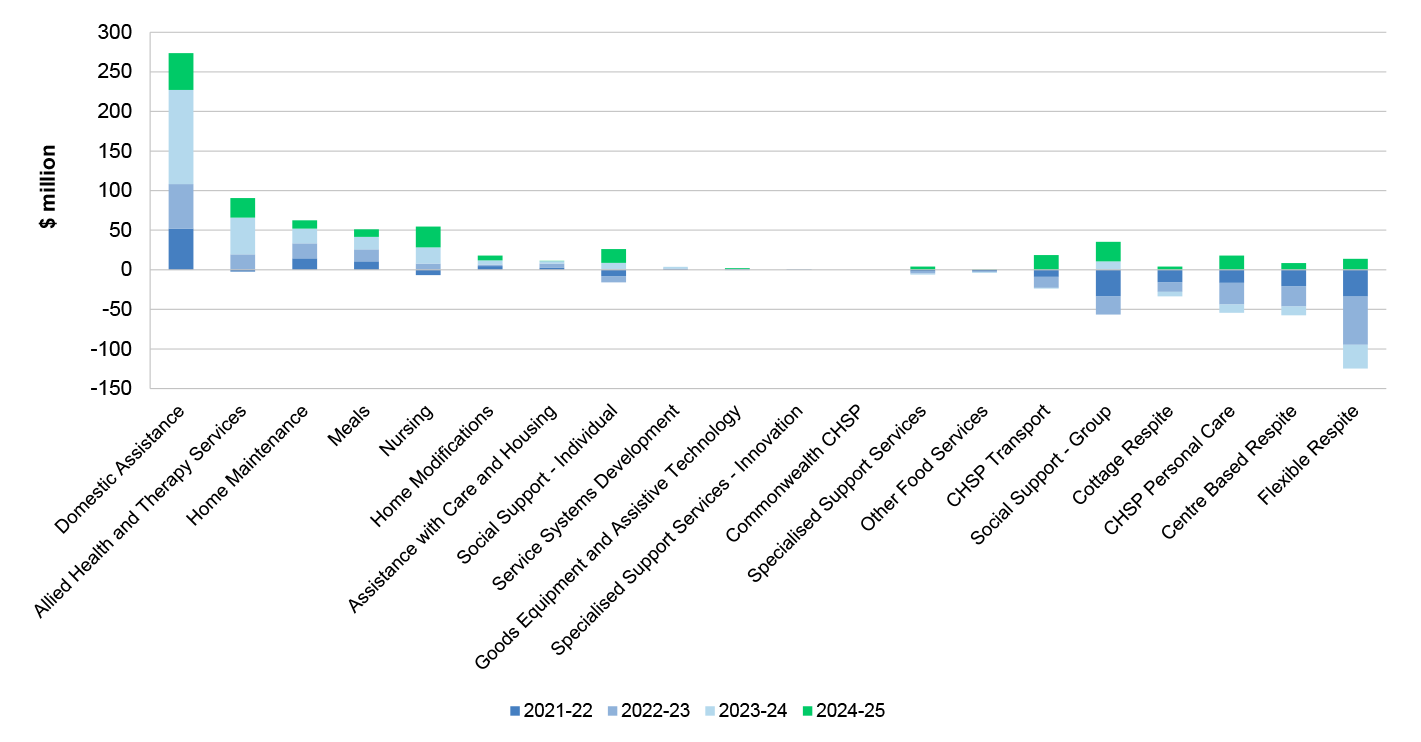
Note a: Analysis does not account for any carry forward amounts (unexpended amounts brought forward from the previous year to be used on top of the funding that has been allocated for the current year). DHDA advised the ANAO in April 2026 that for 2024–25 data, 1.5 per cent of acquittals had not been completed.
Note b: Less than zero indicates underspend. Greater than zero indicates overspend
Source: ANAO analysis of DHDA data.
2.24 A 2023 DHDA survey completed by 125 providers (63 per cent response rate) on CHSP flexibility provisions for five service types found that 70 per cent of providers utilised flexibility provisions to use allocated funds to provide a different CHSP service, where funds allocated for that service were exhausted. On 4 December 2024 the Minister agreed to the tightening of flexibility provisions for assistive technology and home modification service types, meaning that CHSP providers could not reallocate funding to or from these service types without DHDA approval. The brief to the Minister stated that funding for these service types should be controlled over the period 2025 to 2027 so that the funding could be transitioned to a new Assistive Technology and Home Modifications scheme within the Support at Home program47, rather than re-allocated to other services within the CHSP.
2.25 In March 2021 the Royal Commission into Aged Care Quality and Safety made a range of observations about in home care, including that the centralised grants administration process for the CHSP, without a sufficient understanding of local conditions, had led to gaps and inconsistencies in planning, development, management and delivery of services. The systems, data and tools described in paragraph 2.20 support the potential analysis of underspend and overspend by service type, state and territory, Modified Monash remoteness classification48 and Statistical Area Level 2.49 Underspend and overspend is not monitored in the monthly performance report or HSOB data dashboard at this level. DHDA does not use analysis of overspends and underspends to inform its planning, which ‘occurs on a case-by-case basis associated with each CHSP growth funding round’ (see paragraph 2.7).
2.26 The systems, data and tools described in paragraph 2.20 support the potential analysis of underspend and overspend for Aboriginal and Torres Strait Islander and CALD people. DHDA monitors the number of Aboriginal and Torres Strait Islander people and CALD people receiving services at the national level in the HSOB data dashboard. DHDA does not monitor underspend and overspend for these cohorts in the monthly performance report and does not have suitable data to support analysis for other cohorts identified as having diverse needs and requiring tailored support in the 2025–27 CHSP Manual (such as those who are financially or socially disadvantaged, homeless, veterans or LGBTIQA+).50
Forecasting
Future demand for Commonwealth Home Support Program services
2.27 The Australian Bureau of Statistics reported that there was a 52 per cent increase in the number of people aged 65 years and older between 2009 and 2022.51 Eighty-four per cent of CHSP providers and seven of nine peak bodies responding to an ANAO survey (see Appendix 4 and Appendix 5) agreed or strongly agreed with the statement ‘My organisation expects an increase in demand for CHSP services over the next two years’. DHDA’s 2024–25 Annual Report refers to the continued growth in the population of those over 65 in Australia, and states that by 2034, 1.5 million older people will want aged care services to come to them in their homes.52
2.28 In July 2025 DHDA published a report describing the ‘demographic landscape’ of in home care including: over the past 20 years, an increase in the proportion of older people using home care (from 1.4 per cent of 70 to 99 years olds in 2004 to 7.8 per cent in 2024); an increase in CHSP clients from 816,132 in 2022–23 to 834,981 in 2023–24; and a decrease in the number of CHSP providers from 1,334 in 2022–23 to 1,264 in 2023–24. 53 Government funding for the delivery of CHSP services was estimated to be $4 billion in 2027–28. The report included estimates of the ageing population over the next 20 years and forecast CHSP expenditure and demand to 2044. By 2044, it was forecast that approximately 1,820,000 people would be demanding in home care, representing an average annual growth rate of 2.4 per cent. Other research has identified similar trends including an ageing population, increased frailty and chronic illness prevalence, and a strong preference for people to age in place (at home, connected to community).54
2.29 In May 2025 DHDA established ‘Aged Care Service Demand Projection’ guidance ‘to describe the methodology (assumptions and calculations) for calculating future demand for aged care services by service type’. A forecasting methodology was established in the guidance for the Home Care Packages Program and the CHSP. For the CHSP, the forecasting methodology was defined as including estimates of national demand (defined as CHSP expenditure divided by unit cost), latent demand (defined as the cohort of people with a need for care who are not receiving aged care and have not expressed their demand for care) and applying regression models to forecast future overall demand.
2.30 DHDA has one corporate plan measure for the CHSP against which it publicly reports in its annual performance statements (see paragraph 4.9), which is the number of people accessing CHSP each year. DHDA increased the target for this measure from 840,000 in 2024–25 to 860,000 in 2025–26, advising the ANAO in July 2025 that the increase of 20,000 people in the 2025–26 target was based on the amount of growth funds available. There is no evidence that the May 2025 methodology has been used by DHDA to plan or forecast future demand for the CHSP.
2.31 In August 2025 the Aged Care Governance Committee (see paragraph 3.18) received a paper proposing a new and different demand model for the CHSP. DHDA advised the ANAO in October 2025 that the new demand model was in the first phase of development.
Future market capacity for supplying Commonwealth Home Support Program
2.32 Some of the questions in the ANAO surveys of providers and peak bodies examined the perceived sustainability of CHSP service provision (Box 4), which found that almost half of providers and the majority of peak bodies did not agree that CHSP services are sustainable.
|
Box 4: ANAO surveys — supply of Commonwealth Home Support Program services |
|
In relation to sustainable supply into the future:
The most common themes raised by providers relevant to sustainable supply were insufficient and/or inflexible funding (including failure to take into account the service delivery context, such as travel requirements, thin markets and workforce shortages in regional and remote locations), demand for services exceeding providers’ capacity to deliver, and challenges attracting and retaining workers. For example, in response to a question about any specific issues or challenges impacting the effective delivery of CHSP services, key themes included the following.
Providers described a reliance on cross-subsidisation and flexibility provisions; volunteers; adjusting service hours; and ceasing or modifying services. |
Note a: Providers delivering services in the ACT, Northern Territory (NT) and Tasmania were less likely than average to agree or strongly agree that ‘CHSP’ services are sustainable (38, 40 and 41 per cent respectively). Providers delivering services in large rural towns and remote communities were also less likely than average to agree.
2.33 In 2025 DHDA prepared aged care workforce supply modelling for residential and in home aged care (comprising the Home Care Packages Program and the CHSP) based on the 2023 Aged Care Workforce Provider Survey (see paragraph 2.19). This included the combined total workforce and separate modelling for enrolled nurses, registered nurses, nurse practitioners and personal care workers. The modelling forecast 19 per cent growth between 2025–26 and 2031–32 of the home care and support workforce.
2.34 In November 2024 DHDA established terms of reference for an Aged Care Workforce Committee55, which state that the committee is responsible for providing advice on actions that can be undertaken by government and stakeholders to build, train and support the aged care workforce and achieve the desired future state of the aged care workforce. The Aged Care Workforce Committee met nine times between September 2023 and July 2025. Minutes and action items were documented for each meeting. For example, on 13 June 2024 the committee discussed the Home Care Workforce Support Program, noting that the program had met its target of bringing 13,000 new workers into the sector and that the program was being refined to target workers in regional, remote and rural settings. The committee had regular discussions on matters relating to aged care worker registration, training and support. For example, on 13 February 2025 the committee discussed the suitability of vocational qualifications for home care, noting that these qualifications were skewed towards residential care settings. Action items and their status were documented and typically involved committee members undertaking to provide or review papers and reports for the purposes of consolidating feedback. DHDA is a member of the Department of the Prime Minister and Cabinet’s (PM&C) Care and Support Economy Working Group, which has the role of promoting whole-of-government consideration of policy design and implementation relating to the support economy workforce. The working group scheduled eight meetings between May 2025 and December 2025. DHDA advised the ANAO in April 2026 that DHDA officials attended these meetings and that minutes were not taken.
2.35 Between August 2021 and October 2025, DHDA undertook two CHSP provider surveys on matters relevant to estimating the future provider market in the context of the transition of the CHSP to the Support at Home program.
- In August 2021, a ‘2022–23 CHSP extension readiness survey’ that was completed by 800 CHSP providers (57 per cent response rate) examined sector readiness for ‘payment in arrears’ arrangements under the Support at Home program (see paragraph 1.15). The survey found 80 per cent of providers had a long-term plan to deliver aged care services.
- In October and November 2024, a ‘2025–27 CHSP extension stakeholder survey’ completed by 902 CHSP providers (66 per cent response rate) found:
- providers were concerned regarding the long-term viability of small and rural service providers under proposed funding and reporting models;
- there were additional challenges coordinating culturally appropriate care for Aboriginal and Torres Strait Islander and remote clients; and
- eight per cent said they may or would relinquish all CHSP services from 1 July 2025.
2.36 KPMG’s 2025 Aged Care Market Analysis anticipates more new providers entering the home care and support market; further consolidation among existing providers; and a more dynamic provider market with increased competition.56
2.37 DHDA has no documented methodology for forecasting or modelling the supplier market, either nationally or for specific geographic regions, cohorts or service types. DHDA has not documented any estimates of the future supplier market.
2.38 In December 2023 DHDA held a webinar with CHSP stakeholders stating that the staged implementation of aged care reforms would mitigate risks of CHSP provider failure.57 DHDA has not established a CHSP stakeholder engagement plan, strategy or similar (see paragraph 3.6) and does not have regular processes for obtaining CHSP provider input on provider’s capacity to supply CHSP services.
Recommendation no.1
2.39 The Department of Health, Disability and Ageing implement appropriate measurement and monitoring of demand and supply pressures to support advice, decision-making, and planning for the Commonwealth Home Support Program, including as it transitions to the Support at Home program.
Department of Health, Disability and Ageing response: Agreed
2.40 The department is progressing work to improve visibility of CHSP demand and demographic information by Aged Care Planning Region, and/ or other relevant geographical classifications, to better support advice, decision-making and planning, including in the context of the program’s transition to Support at Home.
2.41 The department will continue to improve the use of data and evidence to enhance visibility of demand trends, service utilisation and emerging pressures across regions. This work will be supported by broader efforts to uplift demand and market modelling capability across aged care programs, including CHSP, to inform medium and long-term planning and transition considerations.
Are services provided to eligible people when they are needed?
Upon commencement of the Aged Care Act 2024 on 1 November 2025, CHSP services were being provided to over 100,000 clients without a clear understanding of their needs as they have never been assessed for aged care services. This is not consistent with requirements under the Aged Care Act 2024 — a risk that DHDA is managing. Analysis of all aged care assessments shows that time elapsed between applying for an aged care assessment and completing the assessment increased from 12 days in 2017–18 to 27 days in 2024–25 at the 50th percentile. At the 90th percentile, the number of days increased from 67 to 172. For CHSP clients specifically, the elapsed time between referral to an assessment organisation and a completed assessment in 2024–25 was 21 days at the 50th percentile and 103 days at the 90th percentile. DHDA does not monitor the timeliness of the complete journey from assessment through to receipt of services from CHSP providers, due in part to system and data limitations. DHDA has some data that allows it to monitor time elapsed between a CHSP provider accepting a referral and providing a service but does not regularly analyse or monitor this. DHDA has not established timeliness benchmarks or targets for CHSP service delivery. Forty-two per cent of CHSP clients surveyed by the ANAO did not consider waiting times to receive aged care services in their home to be reasonable, and 51 per cent stated that it was somewhat or very difficult to ‘receive aged care services in your home when you need them’.
2.42 My Aged Care is a contact centre and website that serves as the starting point for access to government-subsidised aged care services.58 People seeking access to CHSP services are required to apply through My Aged Care and complete an assessment to determine individual care needs. Applicants may be recommended to and receive referrals for multiple services where they have an assessed need. A reassessment may be required when an individual’s circumstances have changed significantly. The CHSP provider develops a Support Plan. DHDA’s process for assessing individual need and referring people for aged care services is set out in the 2025–27 and earlier versions of the CHSP Manual and the My Aged Care Assessment Manual (Figure 2.2).59
Figure 2.2: Aged care assessment, referral and service delivery processa
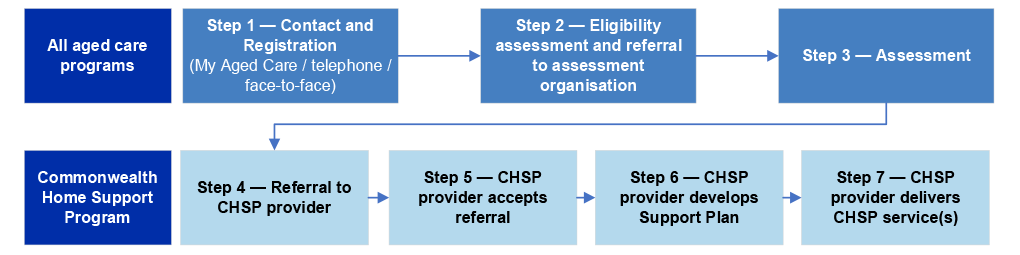
Note a: My Aged Care can refer a client directly to a CHSP registered provider if there is an immediate risk to the older person’s health or safety and services are not available through other means.
Source: ANAO analysis.
Eligibility
2.43 In October and November 2024, a ‘2025–27 CHSP extension stakeholder survey’ with a 66 per cent response rate (see paragraph 2.35) found that 28 per cent of providers reported offering services to individuals without an active assessment referral.60 Based on these survey results, DHDA estimated that approximately 113,000 people received CHSP services in 2023–24 who were not registered with My Aged Care and had not been assessed for CHSP services.6162 DHDA advised the ANAO in November 2025 that this occurred because of: clients being ‘grandfathered’ into the CHSP in 2015; clients having received emergency services without an assessment; clients approaching CHSP service providers directly; registration and assessment challenges for vulnerable clients; and CHSP providers being non-compliant with program guidelines by accepting clients ‘off system’.
2.44 Under the Aged Care Act 2024, CHSP participants need to have been assessed as eligible for the CHSP before services can commence (except in some emergency situations). In March 2025, DHDA established a CHSP ‘client transition project’ to address, in part, the registration and assessment of the unregistered client cohort. In March 2025, DHDA hosted a webinar for CHSP providers, identifying that this client cohort would need to be assessed in order to continue to receive services before the commencement of the Aged Care Act 2024. DHDA requested providers to contact their unregistered and unassessed clients that were receiving and still needed CHSP services and support them to have an aged care assessment, as DHDA did not have the contact details for these clients. DHDA advised the ANAO in November 2025 that it is actively engaging with providers who have requested support to assist vulnerable cohorts of clients to be registered and assessed, and that assessments may take ‘several months’ to complete, but that it does not have full visibility of the actual number of unassessed clients. As discussed in Table 3.3, CHSP providers are required to provide an annual declaration stating that CHSP funds are only expended on clients that have a completed aged care assessment.
Recommendation no.2
2.45 The Department of Health, Disability and Ageing ensure compliance with the Aged Care Act 2024 by accurately quantifying the total number of unregistered clients, establishing a plan to ensure all Commonwealth Home Support Program clients have an aged care assessment, and setting a date for when this work is to be completed.
Department of Health, Disability and Ageing response: Agreed
2.46 The department is working through a staged implementation to support and monitor CHSP provider compliance with the Aged Care Act 2024 (the Act), including the requirement that providers only deliver services to clients who are approved for funded aged care services.
2.47 Before the commencement of the Act, a range of communication activities were undertaken to support providers with unregistered clients. A range of resources was published, including an updated Program Manual outlining requirements under the Act. To support providers transitioning to the Act, the department established a process to manage a limited cohort of unassessed CHSP clients under the exceptional circumstances provision of the Act (subsection 65(4)). These circumstances include situations such as homelessness or significant barriers to engagement with government services.
2.48 The department has strengthened data quality and monitoring through enhancements to the Data Exchange. From 1 January 2026, monthly Data Exchange reporting data includes My Aged Care IDs and providers must record all IDs by 30 June 2026. Using this data, the department will monitor provider reporting to identify unregistered clients and undertake compliance-led engagement where required. The department will be able to quantify the total number of unapproved clients (if any) by early 2027.
Timeliness
2.49 A 2025–27 CHSP extension stakeholder survey undertaken in October and November 2024 found that providers believed there were situations where waiting for the standard assessment and referral process could negatively affect client outcomes, especially in cases requiring short-term or emergency services.
2.50 DHDA does not have systems or a framework for monitoring timeliness at all of the assessment and service delivery steps outlined in Figure 2.2. Although DHDA has targets for timeliness between steps 2 and 3 (see paragraph 2.52), it has not established benchmarks or targets for timely assessment and delivery of CHSP services across the entire client journey from steps 1 to 7. DHDA and CHSP providers separately capture information about clients in different unintegrated systems that do not capture the same unique identifiers to link assessment, referral and service delivery information.
2.51 In November 2024 DHDA advised the Minister for Aged Care on a proposed enhanced data collection and payment assurance process for the CHSP that would require CHSP providers to collect unique aged care ID numbers for CHSP clients. This would support matching of assessment and service delivery data. The Minister agreed to phase in the collection of aged care ID numbers. The collection of My Aged Care IDs commenced in January 2026. Analysis undertaken in January 2026 showed that 356 (30 per cent) of 1,200 providers analysed had My Aged Care IDs for 100 per cent of their clients, while 300 (25 per cent) did not have My Aged Care IDs for any of their clients.
2.52 The Productivity Commission reports elapsed time between steps 2 and 3 at the 50th and 90th percentile at the national level for all aged care assessments through the Report on Government Services.63 In 2022–23, 2023–24, and 2024–25, DHDA reported in its annual reports on timeliness between steps 2 and 3, which found that wait times for home support (the CHSP and Home Care Packages Program combined) were not achieving targets.64 The March 2026 Aged Care Assessment Manual includes key performance indicators for assessment providers that align with the annual report targets. These will be enforceable from 1 July 2026.65 DHDA obtains some qualitative information relating to aged care assessment wait times via intelligence reports (see paragraph 2.16), which indicated issues around assessment wait times (steps 1 to 3) across all states and the NT.
2.53 DHDA maintains systems and data to support internal analysis on timeliness between steps 5 and 7. In 2022–23 and 2023–24, DHDA undertook some ad hoc analysis of timeliness between steps 5 and 7, which found that median days were 19 in 2022–23 and 14 in 2023–24 at the national level. This is not publicly reported.
2.54 Box 5 provides results from ANAO surveys of CHSP clients, providers and peak bodies about timeliness. The survey data shows that more clients disagreed than agreed that waiting times to receive aged care services in their home were reasonable, and that most peak bodies and a significant minority of providers did not agree that providers had the capacity to provide services with little or no waiting period.
|
Box 5: ANAO surveys — timeliness of Commonwealth Home Support Program service delivery |
|
The ANAO surveys (see Appendix 4, Appendix 5 and Appendix 6) found:
|
2.55 DHDA does not undertake structured analysis of complaints about wait times made to it or to the Aged Care Quality and Safety Commission, and does not obtain consolidated data or analysis on complaints from the commission. DHDA advised the ANAO in September 2025 that ‘complaints data’ referred to in advice to government was based on a consideration of ministerial and email correspondence received from older people that identified the service types they had been unable to access or were waiting long periods to access.
2.56 Monitoring or analysis of assessment, referral and service delivery timeliness does not occur at all between steps 1 to 2 or steps 3 to 5. With regard to steps 4 to 5, DHDA does not maintain or monitor waitlists for CHSP services, and CHSP providers are not required to provide this information. The CHSP Manual states that where CHSP providers choose to accept people to ‘very short-term’ waitlists, this is a provider business decision. DHDA publishes quarterly reports on the Home Care Packages Program that includes the number of new packages released, the total number of people accessing a package and the number of people on the National Priority System66 approved for, but waiting to access, a package at their approved level. There is no equivalent information for the CHSP.
2.57 ANAO analysis of aged care assessments for CHSP clients (a subset of the data published by the Productivity Commission) shows that the median elapsed calendar days between referral and assessment (steps 2 to 3) for CHSP clients assessed during 2024–25 was 21 days (19 days for Aboriginal and Torres Strait Islander people; 21 days for people born overseas; 21 days for metropolitan areas; and 16 days for very remote communities) (Table 2.2). At the 90th percentile, elapsed days was 103. Twelve per cent (or approximately 43,000 people assessed for CHSP services in 2024–25) waited more than three months for an assessment.
Table 2.2: Elapsed calendar days between referral to an assessment organisation and a completed assessment for CHSP clients (steps 2 to 3), 2024–25a
|
Modified Monash remoteness classification levelb |
All CHSP clients |
Female clients |
Male clients |
Aboriginal or Torres Strait Islander clients |
Clients born overseas |
||||||||||
|
|
Calendar days |
||||||||||||||
|
|
Mean |
50th |
90th |
Mean |
50th |
90th |
Mean |
50th |
90th |
Mean |
50th |
90th |
Mean |
50th |
90th |
|
Metropolitan |
44 |
21 |
113 |
44 |
21 |
116 |
43 |
20 |
111 |
42 |
19 |
116 |
48 |
22 |
133 |
|
Regional centres |
38 |
21 |
93 |
38 |
21 |
95 |
38 |
21 |
92 |
36 |
20 |
87 |
39 |
21 |
96 |
|
Large rural towns |
36 |
21 |
89 |
36 |
21 |
90 |
35 |
21 |
87 |
37 |
21 |
95 |
37 |
21 |
92 |
|
Medium rural towns |
36 |
21 |
85 |
36 |
21 |
85 |
35 |
21 |
84 |
35 |
20 |
84 |
38 |
21 |
94 |
|
Small rural towns |
36 |
20 |
86 |
36 |
21 |
89 |
35 |
20 |
85 |
35 |
20 |
84 |
37 |
21 |
90 |
|
Remote |
28 |
19 |
68 |
28 |
19 |
67 |
28 |
19 |
69 |
24 |
15 |
59 |
28 |
19 |
70 |
|
Very remote |
24 |
16 |
55 |
24 |
15 |
55 |
24 |
16 |
55 |
22 |
14 |
57 |
25 |
19 |
57 |
|
Australia |
41 |
21 |
103 |
41 |
21 |
104 |
40 |
20 |
99 |
36 |
19 |
91 |
46 |
21 |
120 |
Note a: All CHSP clients that received an assessment.
Note b: See paragraph 2.21 for more information about Modified Monash remoteness classification levels: MM 1 — Metropolitan areas; MM 2 — Regional centres; MM 3 — large rural towns; MM 4 — Medium rural towns; MM 5 — Small rural towns; MM 6 — Remote communities; and MM 7 — Very remote communities. ANAO analysis of remoteness is based on the Modified Monash (MM) Model, which in turn is derived from the Australian Statistical Geography Standard (ASGS). Location mapping was built via linkage of location data (suburb, postcode, state) with the relevant classifications in the ASGS, namely the mesh-blocks and statistical areas, which in turn could be linked with the relevant MM levels. Where there was more than one MM classification associated with the CHSP client location, the more remote classification was selected, to avoid underrepresentation of remote areas in the ANAO’s analysis.
Source: ANAO analysis of aged care assessment data 2024–25.
Recommendation no.3
2.58 To help determine whether Commonwealth Home Support Program services are being provided to people when they are needed and to inform program planning for the Support at Home program, the Department of Health, Disability and Ageing establish monitoring arrangements and benchmarks that allow it to assess and report on the timeliness of Commonwealth Home Support Program service delivery across the entire journey from first contact to service receipt.
Department of Health, Disability and Ageing response: Agreed
2.59 Subject to the decision of Government regarding the future direction and management of the CHSP, the department will establish monitoring arrangements and benchmarks to assess and report on the timeliness of CHSP service delivery across the client aged care journey.
2.60 The department will build on its existing analysis of assessment timeliness to develop a more systematic, end-to-end view of service delivery timeframes. This work will be supported by improved data availability arising from digital transformation initiatives under the Aged Care Act 2024, including enhanced provider reporting through the Data Exchange.
3. Delivering services effectively
Areas examined
This chapter examines whether Commonwealth Home Support Program (CHSP) services are delivered effectively
Conclusion
An ANAO survey of more than 10,000 CHSP clients found that the majority were satisfied with their overall experience of CHSP services. DHDA’s assurance arrangements have focused on service provider reconciliation of grant funds based on provider self-reporting, not on the quality of service delivery, and are reactive. Stakeholder engagement does not fully support continuous improvement in service delivery, in part because there is little engagement with CHSP clients or about the client experience. There are oversight committee arrangements, but there is no program-level assurance framework for the CHSP and DHDA does not plan assurance activities to align with program risks. DHDA has not obtained appropriate assurance that CHSP services are delivered to people based on assessed need. DHDA obtains some information about service quality through delivery partners but does not have assurance over the quality of CHSP service delivery for the majority of providers. DHDA has not analysed complaints or identified lessons learnt from the CHSP to inform its transition to the Support at Home program.
Areas for improvement
The ANAO made four recommendations aimed at DHDA developing a stakeholder engagement plan; establishing and implementing a risk-based assurance framework that considers the quality of CHSP service delivery; and clarifying assurance roles and responsibilities. The ANAO suggested that DHDA could improve or implement project assurance planning, complaints analysis, and a lessons learnt register to inform the transition of the CHSP to the Support at Home program.
3.1 Effective delivery of services in the CHSP requires DHDA to have assurance over providers’ service delivery quality to older people.
3.2 The object of the Aged Care Act 2024 includes:
- ensuring that individuals accessing aged care services are free from mistreatment, neglect and harm from poor quality or unsafe care; and
- providing a robust and risk-based regulatory framework for the delivery of funded aged care services, including accessible complaint mechanisms, that will promote public confidence and trust in the Commonwealth aged care system.67
3.3 The Charter of Partnerships and Engagement was agreed by the Secretaries Board in 2023.68 It aims to support the Australian Public Service to engage meaningfully with people and communities to develop more fit-for-purpose policies and services.69
3.4 The Secretary of the Department of Health, Disability and Ageing (DHDA) has a duty under section 16 of the Public Governance, Performance and Accountability Act 2013 to establish and maintain appropriate internal controls and systems of risk oversight and management.70 The Commonwealth Risk Management Policy sets out the mandatory requirements for managing risks in undertaking the activities of government. Effective risk management supports improved decision making, enhanced management of uncertainty and better delivery of government services.71 The Commonwealth Grants Rules and Principles 2024 state that officials achieve value with relevant money in grants administration by adopting an active risk identification and engagement approach, and through ongoing monitoring and management.72
Does stakeholder engagement support continuous improvement in service delivery?
DHDA has not established a CHSP stakeholder engagement plan to support meaningful engagement with people and communities to develop a fit-for-purpose program. DHDA provided three updates on the CHSP to older people, their families and carers between November 2022 and June 2025. Stakeholder engagement activities for the CHSP have focused on CHSP providers, and there has been limited to no focus on higher levels of stakeholder engagement (involvement, collaboration and empowerment) with any stakeholder groups. In ANAO surveys of CHSP providers and peak bodies, 37 per cent of providers agreed or strongly agreed DHDA had sought feedback on how the CHSP could be improved; and one of nine peak bodies agreed DHDA has engaged with CHSP clients, carers and representatives on their views of the effectiveness of CHSP service delivery. This is not consistent with the DHDA’s aged care engagement principles. Stakeholder engagement practices do not fully support DHDA to understand or improve the quality of CHSP service delivery.
Stakeholder engagement planning
3.5 DHDA has a Stakeholder Engagement Framework, which includes five steps for stakeholder engagement. The first three steps focus on planning and designing the engagement.
3.6 DHDA does not have a stakeholder engagement plan for the CHSP.
3.7 While DHDA does not have a stakeholder engagement plan for the CHSP, between July 2022 and November 2025, DHDA developed communication plans for 10 CHSP activities (for example, a grant extension webinar), including two larger pieces of work in 2025 (the transitioning of unassessed CHSP clients to obtaining an aged care assessment (see paragraph 2.42) and the launch of a new CHSP regulatory model under the Aged Care Act 2024). Between July 2022 and June 2025, DHDA developed five communication plans relating to broader aged care reforms including to home support, which do not specifically identify the CHSP.
Engagement with Commonwealth Home Support Program stakeholders
3.8 DHDA has five aged care engagement principles (purposeful, inclusive, timely, transparent, and respectful), which are mapped against DHDA’s five engagement principles identified in a publicly available Stakeholder Engagement Framework (see paragraph 3.5)73 The purpose of the Aged Care Engagement Principles, which are not made publicly available, is:
Older people and their families and carers are at the centre of our engagement, ensuring our policies and systems respond to the needs of people who need and use aged care.
3.9 Guidance published to support the implementation of the Charter of Partnerships and Engagement identified six engagement methods across a continuum, ranging from ‘sharing’ at the lowest level to ‘empowering’ at the highest level. Similarly, DHDA’s Stakeholder Engagement Framework identified five levels of engagement, from ‘informing’ at the lowest level to ‘consulting’, ‘involving’, ‘collaborating’ and ‘empowering’ at the highest level.
3.10 In November 2022, DHDA published the first edition of EngAged, a monthly e-newsletter for older people, their families and carers on aged care and ageing well. Since November 2022, three editions of the newsletter have provided information on the CHSP. There were higher-level engagement activities with older people, families and carers about the new Aged Care Act and transition of the CHSP to the Support at Home program (including webinars, surveys and consultation on the legislation), however the CHSP was not a specific focus in the engagement between November 2022 to November 2025. DHDA did not have regular scheduled engagement with the peak bodies representing older people, carers and families in relation to the CHSP. From July 2025, monthly meetings with Ageing Australia, a peak body representing providers, were held on ‘CHSP issues and solutions’.
3.11 In September 2025, the ANAO invited 19 peak bodies to provide feedback on the CHSP through an online survey (see Appendix 5). In total, representatives of nine peak bodies (47 per cent response rate) completed the survey. Survey results from questions relating to engagement with clients are shown in Box 6. The survey found that most peak bodies did not believe that DHDA was engaging effectively with stakeholders about the CHSP.
|
Box 6: ANAO surveys — client engagement |
|
In an ANAO survey of peak bodies (see Appendix 5):
One peak body responding to the survey (the Older Persons Advocacy Network) stated: There does not appear to have been any attempt to meaningfully engage with CHSP clients and their carers to understand the value and potential of the program from a consumer perspective. In a client survey, 53 per cent of clients said that they had suggestions for improving the CHSP. Of those providing a suggestion, 16 per cent said that communication could be improved and more support could be provided to navigate the aged care system (see Appendix 6). |
Note a: Four of nine were unsure, and three of nine disagreed.
3.12 Between July 2022 and November 2025, DHDA engaged with individual CHSP providers on management of their grant agreements; engagement on pilot programs supporting the transition to the Support at Home program74; and as part of engagement with the broader aged care sector on aged care reforms.75 In addition to this broader engagement, between 1 July 2022 and 30 June 2025, there was some regular engagement with CHSP providers for matters specifically relating to the CHSP, comprising:
- from October 2022, a ‘Your aged care update’ newsletter published weekly by DHDA;
- from November 2022, an online forum for sector support and development providers’ community of practice76;
- from 2024, the Meals on Wheels Australia and the Commonwealth Forum to ‘bring together key stakeholders involved in meal services [to] … provide a platform for collaboration and open dialogue about pressing issues within the sector’77; and
- from March 2024, a monthly ‘Working in aged care update’ newsletter.
3.13 For matters specifically relating to the CHSP, there was also some engagement with CHSP providers on an ad hoc basis, comprising letters, surveys and webinars. The nature of this regular and ad hoc provider engagement was largely consistent with the two lowest-level ‘inform’ and ‘consult’ engagement practices outlined in DHDA’s Stakeholder Engagement Framework. The ongoing community of practice for SSD providers involved higher-level engagement.
3.14 Between July 2022 and November 2025, DHDA did not undertake consultation with Aboriginal and Torres Strait Islander people or specialist providers specifically about the CHSP.
3.15 In September 2025, the ANAO invited 1,486 employees of 1,168 CHSP providers to provide feedback on the CHSP through an online survey (see Appendix 4). In total, 495 people from 436 provider organisations (33 per cent response rate) completed the surveys. Survey results from questions relating to engagement with providers are provided in Box 7, and showed that most providers did not feel that DHDA was engaging with them effectively to improve the quality of the CHSP.
|
Box 7: ANAO surveys — provider engagement |
|
In relation to engagement with providers, the ANAO surveys found (Appendix 4 and Appendix 5):
Key themes raised in the ANAO provider survey regarding how DHDA works with providers to support effective delivery of CHSP services and meet CHSP objectives included communication and engagement. Providers appreciated regular dissemination of information from DHDA through newsletters and webinars but stated they would like more two-way, tailored and face to face engagement. |
Recommendation no.4
3.16 The Department of Health, Disability and Ageing develop a stakeholder engagement plan for the Commonwealth Home Support Program that:
- identifies stakeholders, engagement objectives and methods;
- considers approaches to ensure successful engagement with diverse audiences;
- includes direct engagement with participants, their families and carers;
- considers higher levels of engagement (involve, collaborate and empower);
- incorporates ongoing review and evaluation of engagement activities; and
- includes the transition to the Support at Home program.
Department of Health, Disability and Ageing response: Agreed
3.17 The department will develop a stakeholder engagement plan for the CHSP that supports meaningful, ongoing engagement with key stakeholders, including service providers, clients, carers and representative bodies, and informs continuous improvement and transition to Support at Home.
Is there a fit-for-purpose framework for assuring effective service delivery?
While the Aged Care Quality and Safety Commission (ACQSC) and the Department of Social Services (DSS) have assurance responsibilities over CHSP service delivery quality, DHDA maintains responsibility for overall program delivery and effectiveness. DHDA has a committee structure to oversee the CHSP and has set out delivery partner roles and responsibilities through memoranda of understanding or similar. DHDA has a planning methodology for program assurance activities, which are intended to give decision-makers confidence that work is progressing as planned and in accordance with legal and policy frameworks. DHDA has not established a risk-based CHSP program-level assurance framework to support assurance planning for the CHSP and has not planned assurance activity in alignment with risk. CHSP projects that have been assessed as ‘tier 1’ (of significant importance to DHDA with a high level of risk, effort and investment to deliver) also do not have assurance plans. This is not consistent with DHDA’s Project Management Framework.
Commonwealth Home Support Program governance arrangements
3.18 DHDA has oversight committees relevant to in home aged care programs (Figure 3.1).
- Aged Care Governance Committee — The Aged Care Governance Committee provides oversight of the Ageing and Aged Care Group within DHDA, including its management of aged care reforms and business as usual activities.
- Aged Care Transformation Program Steering Committee — The committee is responsible for providing oversight, advice and assurance on the implementation of the Aged Care Transformation Program.
- Access and Home Support Program Board — The Board reports to the Aged Care Transformation Program Steering Committee and is responsible for oversight, advice and assurance for three DHDA divisions, including the Access and Home Support Division, which is responsible for the CHSP. Membership comprises representatives of DHDA, DSS, Australian Digital Health Agency, Digital Transformation Agency and Department of Veterans’ Affairs. One member is the Independent Assurance Advisor, who is responsible for advising the Board on reform projects.
- Home Support Operations Board — The Board is responsible for overseeing ongoing CHSP program management. In May 2025, the Chair proposed that the purpose of the Board ‘become more governance focused than [an] information sharing forum. The change will focus on decision-making, and mitigation and management of risks …’. Updates to terms of reference in July 2025 reflected this change in emphasis. Board membership is comprised of DHDA and DSS representatives.
Figure 3.1: Committees with Commonwealth Home Support Program oversight
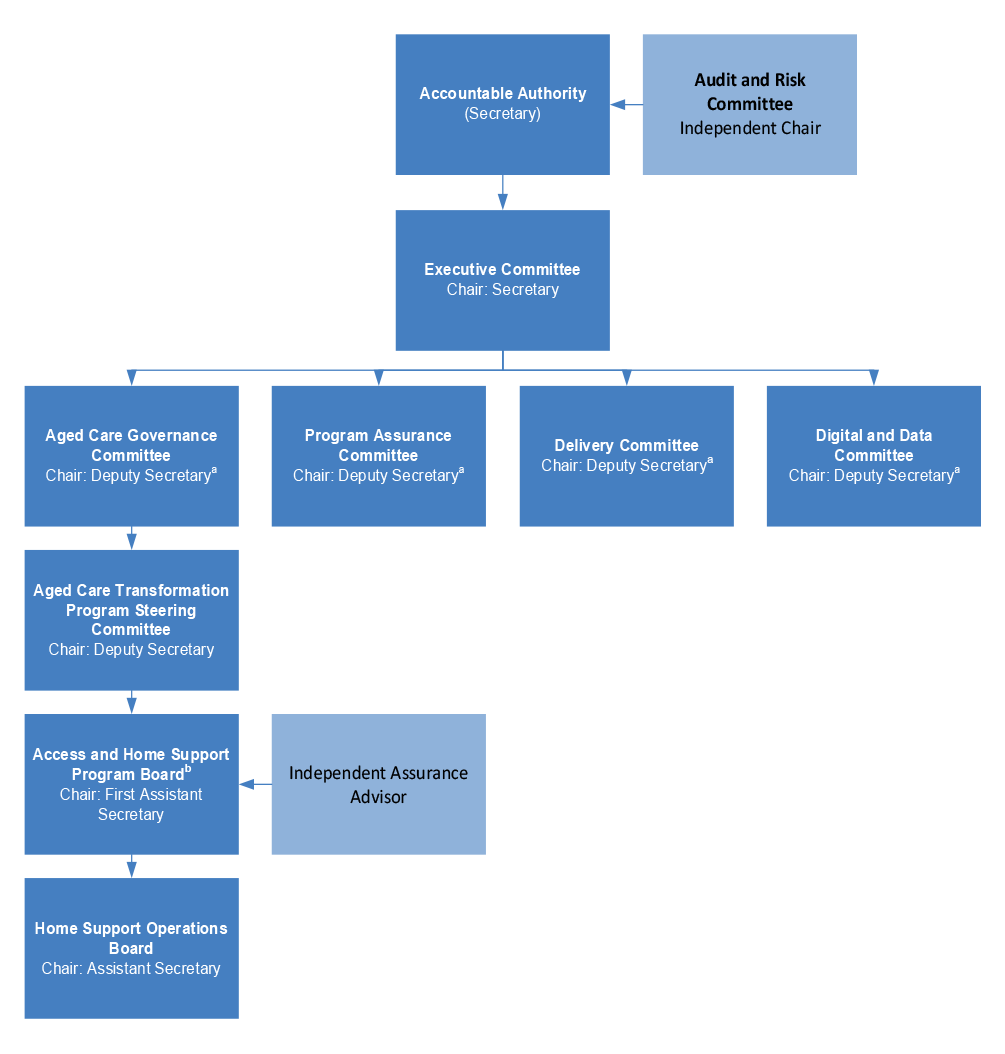
Note a: The committees are each chaired by a different Deputy Secretary.
Note b: The In-Home Aged Care Program Board was renamed the Access and Home Support Program Board in February 2025.
Source: ANAO analysis.
3.19 Although DHDA is responsible for administering the CHSP, two other entities have a role in program delivery: the ACQSC and DSS through the Community Grants Hub. DHDA has a memorandum of understanding (MOU) (June 2024, revised December 2025) with the ACQSC, which identifies entity responsibilities78 and detailed operational requirements. DHDA has a partnership agreement with DSS for the provision of grants administration services, which expires on 30 June 2026(Table 3.1).
Table 3.1: Delivery partner responsibilities and activities, to 31 October 2025
|
|
Department of Health, Disability and Ageing |
Aged Care Quality and Safety Commission |
Community Grants Hub |
|
Primary responsibility |
|
Regulate the performance and compliance of approved providers and the workforce in accordance with legislative frameworks, as applicable to the ACQSC’s scope. Under the Aged Care Act 1997 and the Aged Care Quality and Safety Commission Act 2018 (ACQSC Act), CHSP providers were not required to be an ‘approved provider’ to deliver services. |
|
|
Key activities relating to the CHSP |
|
|
|
Source: ANAO analysis.
3.20 With the commencement of the Aged Care Act 2024 on 1 November 2025, for the first time the CHSP came completely under aged care legislation. This change introduced new responsibilities for CHSP service providers (e.g. abide by the Aged Care Code of Conduct and be registered with the ACQSC before providing CHSP services). Under the new Act, the ACQSC is able to undertake direct regulatory action with CHSP providers, including placing conditions on or revoking a provider’s registration. Some CHSP providers will be audited against the Aged Care Quality Standards, a more thorough assessment process than the previous review arrangements.
3.21 In February 2024, DHDA, ACQSC and DSS established a CHSP ‘program assurance group’ to provide activity updates, which may include feedback from CHSP providers.79 The group met five times between February 2024 and November 2025. Meeting papers identify service delivery issues and challenges. The program assurance group recorded action items for some of the specific operational issues and concerns identified in meetings. Members provided updates through ‘intelligence’ templates, which were consolidated by DHDA into a monthly intelligence report (see paragraph 2.16). A quarterly assurance report, which was provided to the Home Support Operations Board, consolidates the monthly reports and covers three key themes: provider compliance; operational issues and challenges; and program participant trends. The program assurance group does not have terms of reference or a clearly stated purpose. As stated in paragraph 3.18, the Home Support Operations Board revised its terms of reference to have a stronger focus on governance and providing strategic direction and oversight for the CHSP from July 2025.
Department of Health, Disability and Ageing assurance planning
3.22 While the ACQSC and DSS have assurance responsibilities over service delivery quality, both before and after the commencement of the Aged Care Act 2024, DHDA maintains responsibility for overall program delivery and effectiveness. The audit examined DHDA’s assurance over the CHSP, including its actions in response to the ACQSC and Community Grants Hub’s assurance activities.
3.23 DHDA has an entity-wide Assurance Framework (September 2021) that ‘provides detailed guidance for staff at all levels to understand and deliver their assurance responsibilities’ and states that:
Assurance … is designed to provide confidence to leaders and decision makers that aspects of [DHDA’s] business are being managed within expectations and in accordance with legal and policy frameworks.
3.24 A program-specific assurance framework was established for the Home Care Packages Program. There is no equivalent program-specific framework for the CHSP.
3.25 The entity-level Assurance Framework identifies a range of assurance activities that can be undertaken based on the level of assurance confidence needed and sets out a six-phase cycle to prioritise through risk assessment the appropriate assurance activities (Table 3.2). DHDA’s Risk Management Framework distinguishes project risks from program risks (which relate to programs listed under the Portfolio Budget Statement structure).80 The Risk Management Framework states that programs must capture risks in a risk register and monitor controls effectiveness at least annually. For project risks, the risks must be captured in DHDA’s project management tool ‘Altus’ and controls must be monitored for effectiveness at least annually.
3.26 The Assurance Framework and the Risk Management Framework largely have not been applied to the CHSP to plan appropriate program assurance activities (Table 3.2).
Table 3.2: Assurance planning and implementation for the Commonwealth Home Support Program
|
Assurance Framework phase |
Description of phase |
Assessment |
Assessment rationale |
|
Phase 1 — identify assurance needs |
Questions to determine if and how much assurance is needed, relating to risk, executive focus, known issues /weaknesses and change. |
▲ |
DHDA has two out-of-date risk registers that relate to the CHSP.
CHSP-related risks reported to the Access and Home Support Program Board and Home Support Operations Board are framed around specific projects and do not identify strategic risks to the CHSP as a whole, including risks to the achievement of CHSP objectives or service delivery principles. An assessment of assurance needs in order to prioritise assurance activity has not been undertaken for the CHSP. |
|
Phase 2 — understand existing assurance |
Questions to determine if assurance already exists in the form of controls and activities. |
▲ |
In 2024, DHDA prepared an ‘assurance snapshot’ with the intention to ‘document key risks, challenges, priorities, and assurance activities’ and to inform DHDA’s internal audit work program. The snapshot included first, second and third-line assurance activities against six key risks.a The snapshot was not used to plan assurance activities going forward and was not updated. DHDA advised the ANAO in June 2025 that no update was made due to a change in internal audit direction. |
|
Phase 3 — prioritise through risk |
Assurance focus areas to be prioritised through a risk assessment. |
▲ |
In addition to the out-of-date and incomplete CHSP risk registers, the monthly intelligence report (see paragraph 2.16), which is provided to the Home Support Operations Board, identifies issues. The 2024 assurance snapshot described in relation to Phase 2 sets out six key program risks for the CHSP, as ‘outlined by the program [senior responsible officer]’. These are not further assessed in the snapshot. Risks for each of five CHSP projects (paragraph 3.31) were entered into Altus. Between 1 July 2023 and 30 June 2025, the Access and Home Support Program Board received project status updates, which included ‘top risks’ extracted from Altus. In August 2024, a Home Support Operations Board program activity dashboard was expanded to include a summary of top project risks. The risks reported to the Board in 2025 for two projects were inconsistent with those recorded in Altus. |
|
Phase 4 — undertake assurance |
Different types of assurance activities that provide varying levels of assurance confidence (see Figure 3.2). |
▲ |
DHDA’s assurance activities for the CHSP are described in paragraph 3.37 and Figure 3.2. |
|
Phase 5 — report and monitor Phase 6 — implement and refine |
A formal record of assurance activities, outcomes and recommendations will facilitate stakeholder communication and decision-making, and inform future assurance activities. |
■ |
There is no consolidated reporting of program assurance activities for the CHSP. |
Key: ■ Not implemented ▲ Partly implemented ◆ Largely or fully implemented
Note a: DHDA defines first line as the areas responsible for delivery of departmental outcomes, the second line as the department-wide functions that establish common standards and policies and the third line as the dedicated internal audit function that provides independent assurance.
Source: ANAO analysis.
Recommendation no.5
3.27 The Department of Health, Disability and Ageing establish a risk-based Commonwealth Home Support Program assurance framework to support the monitoring of quality service delivery and continuous improvement, including as the Commonwealth Home Support Program transitions to the Support at Home program.
Department of Health, Disability and Ageing response: Agreed
3.28 The department will establish a risk-based program assurance framework for the CHSP, including clear risk ownership and control responsibilities (see the department’s response to recommendation 6). The framework will leverage existing departmental systems to support the identification, reporting and ongoing monitoring of key program risks and controls. To support effective oversight, the department will also review and update its existing governance arrangements and ensure they remain fit for purpose.
3.29 In addition, the department will explore further ICT investment to enhance the Data Exchange system to enable the monitoring of service timeliness. Any additional ICT investment would be subject to Government consideration.
3.30 DHDA’s Project Management Framework requires projects to be classified into one of three tiers based on budget, complexity, risk and impact. Assurance requirements are based on the project tier. Tier 1 projects (which are defined as being of significant importance to DHDA with a high level of risk, effort and investment to deliver) require ongoing assurance from an external assurance provider who reports to the project’s ‘designated governance authority’, Audit and Risk Committee, Program Assurance Committee, Delivery Committee ‘and/or’ the Digital and Data Committee. Tier 2 projects require an assurance plan with scheduled assurance activities performed by an internal or external assurance provider.
3.31 Since July 2023, the Access and Home Support Program Board has received monthly reports on five CHSP projects, two of which were classified as tier 1 projects: extend existing CHSP grant arrangements by 12 months to 30 June 2025 and extend existing grant arrangements by 24 months to 30 June 2027. For the tier 1 30 June 2025 extension project, a draft assurance plan that did not include external assurance was provided to the Access and Home Support Program Board in February 2024 and never endorsed. For the tier 1 30 June 2027 extension project, a project assurance plan was not developed. Two of the other three81 CHSP projects were classified as tier 2 projects. An undated assurance plan was prepared for the tier 2 CHSP client transition project (see paragraph 2.44), which notes that external assurance reviews or audits are to be confirmed. As at December 2025, the plan had not been endorsed by the Access and Home Support Program Board. The other tier 2 project does not have an assurance plan.
Opportunity for improvement
3.32 DHDA could improve controls to ensure that projects have assurance arrangements that are in line with its Project Management Framework.
Is there assurance that services are delivered effectively?
DHDA’s assurance activities for the CHSP have focused on assuring provider expenditure against allocated grants funding, which is based on provider self-reporting. DHDA acts on providers’ financial performance to improve program integrity. DHDA has not obtained full assurance that the right CHSP services are being delivered to people who need them. DHDA receives ACQSC and Community Grants Hub referrals of providers who are non-compliant with quality requirements. DHDA did not cancel any CHSP provider agreements based on the ACQSC’s assessment of non-compliance with the Aged Care Quality Standards in 2023–24 and 2024–25. DHDA has not obtained assurance over the overall quality of CHSP service delivery by the majority of CHSP providers. In an ANAO survey of CHSP providers, 87 per cent agreed or strongly agreed that CHSP services are of high quality. In an ANAO survey of CHSP clients, 65 per cent were satisfied or very satisfied with their overall experience of the services they received in the last six months. There is no analysis of complaints or compilation of lessons learnt to support the transition to the Support at Home program.
3.33 The Aged Care Act 1997 listed the responsibilities of approved aged care providers, which focused on: the quality of care they provide; the user rights of the people they provide care to; accountability for the care provided; and suitability of key personnel. While they did not need to be approved providers, under their grant agreements with DHDA and the CHSP Manual, CHSP providers were required to meet some quality requirements of approved providers including:
- being assessed as compliant under the Aged Care Quality Standards (which are developed by DHDA) by the ACQSC82;
- making reports under the Serious Incident Response Scheme83 to the ACQSC;
- assisting people to understand their rights under the Charter of Rights; and
- ensuring that staff and volunteers have had a National Criminal History Record Check within the last three years.
3.34 The CHSP Manual 2025–27 sets out five CHSP service delivery principles: social and cultural sensitivity; client, carer and family empowerment; client-centred support with a wellness and reablement approach; committed and responsive service provision; and wellness and reablement.84 Part C of the CHSP Manual outlines provider responsibilities relating to quality arrangements, client rights, incident management and staffing.
3.35 The Aged Care Act 1997 did not specify DHDA assurance functions or powers over unapproved providers, such as CHSP providers.85 The Aged Care Act 2024, which took effect on 1 November 2025, gives the ‘System Governor’ (the Secretary of DHDA) the power to conduct assurance activities over ‘registered’ providers.
3.36 A provider compliance framework included as an appendix to the CHSP Manual and first published in June 2024, along with individual grant agreements with CHSP providers, comprise the framework for CHSP provider service delivery assurance. Under the framework, compliance requirements largely focus on financial acquittals of grant funds, and largely do not address quality risks, such as lack of participant choice and control86, or the service delivery principles set out in the Manual.
3.37 DHDA’s entity-level Assurance Framework requires the prioritisation and selection of appropriate program assurance activities, which provide differing levels of assurance depending on the activity’s independence and methodological rigour. Figure 3.2 summarises DHDA’s program assurance activities for the CHSP in 2023–24 and 2024–25 against the Assurance Framework.
- Assurance confidence — Where assurance activities were undertaken, these involved assurance methods with lower levels of assurance confidence.87 Higher confidence could have been achieved through assurance activities such as program evaluation or review (see paragraph 4.25) or surveys (for example, with CHSP participants). Since July 2022, two internal audit reports have been completed for in home aged care programs and activities; neither audit included the CHSP.
- Reporting and data assurance — Assurance activities focused on the expenditure of CHSP grant funding, as determined through providers’ monthly self-reporting (see Table 3.3). DSS provided a data quality statement for CHSP data collected and held by the Community Grants Hub in 2023–24 (see paragraph 4.9), which describes the level of assurance over accuracy and completeness with current controls as ‘moderate’, and that the risk rating with current controls as ‘medium’.88 In relation to the risk of provider fraud89, DSS also stated that the level of assurance was ‘moderate’ and the risk rating was ‘medium’.
- Assurance over service delivery quality — While a focus on client ‘wellness and reablement’ (covered in two of the five service delivery principles) has increased over time (see Table 3.3), DHDA has not established service quality indicators for the CHSP.90 DHDA is unable to determine if CHSP clients are receiving the services that they were assessed as requiring (see paragraph 2.49 and Table 3.3). DHDA has established an escalated provider list to identify and monitor for provider non-compliance and underperformance that considers referrals from the ACQSC and the Community Grants Hub (see paragraph 3.47) and it receives information from the ACQSC on CHSP providers that are non-compliant with the Aged Care Quality Standards (see paragraph 3.46). However, DHDA does not have assurance mechanisms in place to determine the quality of service delivery for most CHSP providers.
Figure 3.2: DHDA’s assurance activities by assurance confidence, 2023–24 to 2024–25
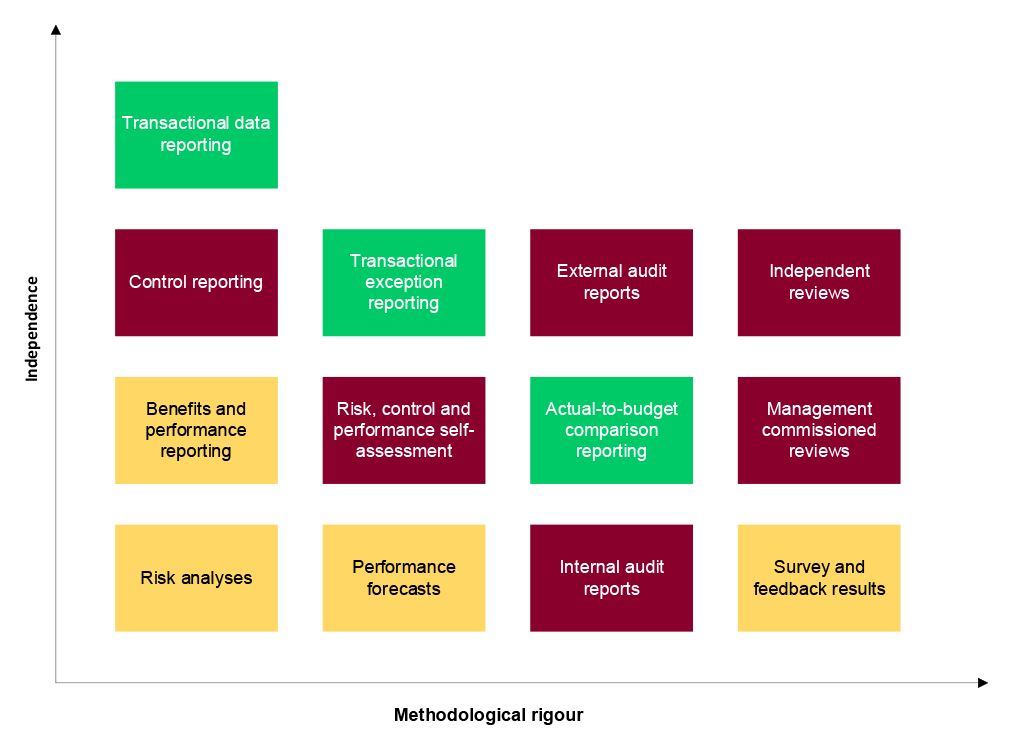
Key: ■ Activity undertaken for the CHSP ■ Some activity undertaken ■ Activity not undertaken for the CHSP
Source: DHDA Assurance Framework and ANAO analysis.
3.38 In addition to the provider and peak body surveys, in November to December 2025, the ANAO invited 159,997 CHSP clients to provide feedback on CHSP services through an online survey (see Appendix 6). In total, 10,125 clients completed the survey (6.5 per cent response rate). Box 8 provides results from survey questions that relate to service delivery quality, and shows that the vast majority of providers and peak bodies representing providers believe CHSP provides high-quality services, and the majority of CHSP clients are satisfied with the services they receive.
|
Box 8: ANAO surveys — effectiveness of service delivery |
|
ANAO CHSP provider and peak body surveys found (see Appendix 4 and Appendix 5):
In an ANAO survey of CHSP clients, 65 per cent were satisfied or very satisfied with their overall experience of aged care services they had received in their home from a local provider through the CHSP in the previous six months, and 18 per cent were dissatisfied or very dissatisfied (Appendix 6). Older clients, clients who did not identify as culturally or linguistically diverse, and clients who did not identify as Aboriginal or Torres Strait Islander were more satisfied on average. The top three reasons people reported being satisfied with CHSP services were: being happy with the service; friendly, respectful or helpful staff; and prompt, reliable or regular services. The top three reasons people reported being dissatisfied with their services were: long wait times, assessment delays and slow follow up; staffing inconsistencies and service cancellations; and providers being at capacity and not taking on new clients. In response to questions about the most recent time they received specific services from their local provider, ‘the kindness and compassion shown by staff’ generated the highest levels of satisfaction on average. Client satisfaction with most recent services received 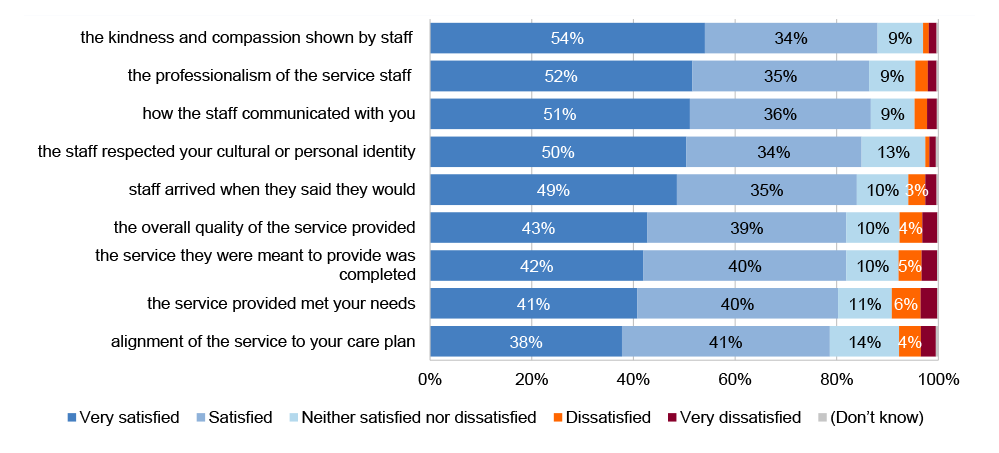
Source: ANAO CHSP client survey. Fifty-three per cent of clients said that they had suggestions for improvement. Suggestions related to quality of service delivery included better follow up and oversight (mentioned by eight per cent), having more staff (eight per cent), having better trained staff (eight per cent), having more staffing consistency (five per cent), and tailoring services to individual needs (six per cent). |
Note: Northern Territory providers were less likely than average to agree or strongly agree that their organisation had established service quality measures or standards (81 per cent).
Reporting assurance
3.39 Section 12.2 of the CHSP Manual states that providers must submit reports outlined in their grant agreements within specified timeframes. CHSP grant agreement reporting requirements and the delivery partner responsible for monitoring the requirements are outlined in Table 3.3. In relation to reporting that DHDA is directly responsible for assuring, DHDA’s assurance is partial.
Table 3.3: DHDA assurance of provider reporting, 2025 to 2027
|
Mandatory requirementa |
Reporting description |
Delivery partner responsible for assurance (CHSP Manual) |
DHDA assurance |
|
Performance report for sector support and development (SSD) activitiesb Biannual |
Reporting on all activities in the approved activity work plan. |
Not specified in CHSP Manual. DHDA advised the ANAO in September and November 2025 that DHDA reviewed the 2022–23 performance reports, the Community Grants Hub reviewed the 2023–24 reports, and the process to review 2024–25 performance reports was still to be confirmed with the Community Grants Hub. DHDA may, by notice withhold payment if the provider fails to submit their report. |
▲ There was evidence of DHDA conducting a review of 2022–23 performance reports. The reports focused on SSD provider activities outputs and issues and did not include information on SSD outcomes. DHDA did not hold records of the results of the Community Grants Hub review of 2023–24 reports. Prior to 2024–25, providers were not required to provide a copy of their activity work plan, meaning there was nothing to hold providers to account against. An activity work plan was required from 2024–25. Between 1 July 2023 and 30 June 2025, DHDA did not issue any notices withholding payment. |
|
Performance report for non-SSD activities Monthly |
Reporting on services the provider is contracted to deliver under the grant agreement, including the location of services delivered and units delivered (e.g. meals or hours). |
The Manual specifies that the Community Grants Hub is required to monitor the reported activity levels against the annual grant funds, with payments adjusted based on actual service provision. The Community Grants Hub notifies DHDA of any providers who fail to submit their report. DHDA may issue a breach notice for providers who fail to submit their report within two months. If a notice is issued, the provider’s monthly payment is suspended until the performance reports are submitted. |
◆ Between January 2023 and December 2024, the Community Grants Hub provided DHDA with a six-monthly summary of engagement activities with providers. Between 1 July 2023 and 30 June 2025, DHDA produced a monthly data report that identified providers that had not met their obligation to submit monthly performance reports. Between 1 July 2023 and 30 June 2025, DHDA issued 11 breach notices. |
|
Performance report — wellness and reablement Annual from July 2018 |
Non-SSD providers were required to report on the implementation of a wellness approach.c The focus in the reporting template on CHSP participant outcomes increased over time. In early 2021, DHDA published guides and tools to assist providers to embed a wellness and reablement approach into their service delivery. |
The Manual states that DHDA is responsible for monitoring submission of the wellness and reablement report. The Community Grants Hub is required to follow up with providers about outstanding submissions, as required. |
◆ DHDA published a ‘wellness and reablement outcome report’ based on provider reports from 2018, 2019–20, 2021, 2022, and 2023. In the first outcomes report in 2018, DHDA stated that provider reports were used to identify implementation issues and supports that may be needed. In the 2023 outcomes report, DHDA stated that the purpose of the provider reports is to measure providers’ progress against embedding a wellness and reablement approach and to gain a more detailed understanding of how wellness and reablement can be delivered in practice. The 2023 report concluded that CHSP providers saw the benefit of embedding wellness and reablement approaches, but found them challenging to implement and maintain. Barriers included capacity, cost, demand and staffing. |
|
Financial acquittal report Annual |
A financial declaration that declares:
2024–25 grant agreements had 4 objectives, including 3 referring to provision of services to ‘eligible’ (assessed) individuals as outlined in the CHSP Manual 2024–25. |
Not specified in the Manual. A December 2024 standard operating procedure states that the Community Grants Hub is responsible for managing the acquittal process and notifying DHDA of providers who fail to submit their financial acquittal report. DHDA may issue a breach notice for providers who fail to submit their report within two months of the due date. If a notice is issued, DHDA may request that the Community Grants Hub suspend payment until a report is received. |
▲ Between 1 July 2023 and 30 June 2025, DHDA issued 16 notices withholding payment. DHDA has not obtained assurance that people accessing the CHSP are eligible — the third part of the financial declaration (see paragraph 2.44). In August 2025, DHDA advised the ANAO that neither DHDA nor the Community Grants Hub check if CHSP participants have been approved for the services they receive. DHDA advised the ANAO in January 2026 that the provider reporting system (DEX) has been upgraded to enable the collection of unique CHSP client identification numbers (My Aged Care IDs, or MAC IDs) to enable DHDA to cross-check the assessment status of people receiving CHSP services. The new reporting field for MAC IDs is optional for providers to complete. DHDA anticipate making this field mandatory by 30 June 2026. In November 2025, DHDA advised the ANAO that provision of CHSP services to unassessed clients is due in part to provider non-compliance with grant requirements. DHDA has not addressed this risk as part of its assurance program. |
|
Child safety statement of compliance Annual from March 2026 |
A statement confirming that services have been delivered in line with the Child Safe Supplementary Term. |
Not specified in the Manual. DHDA advised the ANAO in September 2025 that it will share responsibility for monitoring with the Community Grants Hub. |
Not assessed (commences March 2026) |
Key: ■ No assurance ▲ Partial assurance ◆ Largely or fully assured
Note a: Requirements as specified in 2025 to 2027 grant agreements. In addition, the System Governor may also request a compliance report and/or service delivery report.
Note b: SSD services are delivered to providers to try and increase sector capacity and improve quality of services. SSD services agreements will cease on 30 June 2026.
Note c: DHDA introduced requirements for service providers to increase their focus on activities supporting independence and wellness and to provide more choice to participants. These arrangements did not apply to Victorian CHSP providers in 2018–19.
Source: ANAO analysis of standard CHSP grant agreement, other DHDA documentation and advice to the ANAO.
3.40 In 2022 DHDA piloted a performance review process of selected providers who delivered significantly less than their contracted activities, according to 2021–22 data collected by DSS. This process, known as a ‘Quarter 1 (Q1) review’, was also undertaken by DHDA in 2023 and 2024 with expanded selection criteria to include providers with a history of reporting non-compliance and breach notices.91 The number of providers identified for follow up through this process ranged from 52 in 2022 to approximately 130 in 2023 and 2024, with between 55 per cent and 69 per cent receiving a funding reduction and between one and eight providers relinquishing services after the review. DHDA reported that the total funding returned to the CHSP following Q1 reviews was $74.5 million in total across three years. In August 2025, DHDA established a ‘performance monitor tracker’ that identified CHSP providers that were selected for the 2024 Q1 review process to monitor reported delivery against contracted activities.
Service quality assurance
3.41 DHDA is responsible for the stewardship of the CHSP and ensuring the program is meeting its objectives. The ACQSC is responsible for conducting quality reviews of CHSP providers and monitoring the quality of care and services.92 With the exception of the wellness and reablement reporting requirements outlined in Table 3.4, CHSP provider responsibilities relating to quality are largely monitored or assessed by the ACQSC (against the Aged Care Quality Standards).93
3.42 As for reporting assurance, for several quality elements outlined in the CHSP Manual, the delivery partner responsible for assurance is not stated or is unclear. For example, section 9.2 of the CHSP Manual sets out a requirement for providers to monitor and review participants’ circumstances to ensure service delivery is appropriate but does not specify how providers’ delivery of this requirement will be assured.
Recommendation no.6
3.43 The Department of Health, Disability and Ageing work with the Aged Care Quality and Safety Commission and Department of Social Services to identify and respond to gaps in assigned assurance roles and responsibilities for the ongoing administration of the Commonwealth Home Support Program and its transition to Support at Home.
Department of Health, Disability and Ageing response: Agreed
3.44 The department will work with the Aged Care Quality and Safety Commission (ACQSC) and the Department of Social Services (DSS) to review and clarify established roles and responsibilities to strengthen the administration of the CHSP. This work will refine existing arrangements and establish clear risk owner and control responsibilities across participating entities. The department, working with ACQSC and DSS, will also update governance arrangements to support transparent communication of risks and controls of the program.
3.45 Table 3.4 outlines DHDA’s assurance over provider responsibilities related to quality and accessibility of service delivery where the CHSP Manual clearly indicates this is DHDA’s responsibility.94
Table 3.4: DHDA assurance over provider responsibilities related to quality and accessibility of CHSP service delivery
|
CHSP Manual Section |
Provider responsibility |
DHDA assurance |
|
9.1 |
The Aged Care Quality Standards require providers to demonstrate effective management processes based on a continuous improvement approach. Upon request, providers must provide a plan for continuous improvement, which should include policies for: managing staff and volunteers; regulatory compliance with funded program guidelines; relevant legislation, including Work Health and Safety legislation; professional standards; and complaint mechanisms. |
■ DHDA advised the ANAO in September 2025 that: ‘The department and [Community Grants Hub] have not established formal processes to test and review [continuous improvement plans]. Accordingly, no testing, reviews or outcomes have been undertaken. The department will work with the [Community Grants Hub] on this element as part of managing CHSP provider compliance for [2025 to 2027].’ |
|
10.10 |
The 2024–25 CHSP Manual referred to an Aged Care Workforce Census that was mandatory for providers receiving $35,000 or more in annual grant funding. The census collected information on the CHSP workforce, including staff qualifications and training. The Aged Care Provider Workforce Survey replaced the Aged Care Workforce Census in 2023.a |
▲ There is no requirement on how frequently the survey needs to be conducted and, unlike for the Census, the 2025–27 CHSP Manual does not state that the survey is mandatory for providers selected as part of the survey sample. The CHSP response rate for the 2023 survey was 34 per cent (321 of 941 selected CHSP services). DHDA has not followed up on non-response to the survey. A survey has not been conducted since 2023.b |
Key: ■ No assurance ▲ Partial assurance ◆ Largely or fully assured
Note a: The 2023 survey collected data from a sample of providers delivering residential aged care, the Home Care Packages Program, the CHSP, Multi-Purpose Services and the National Aboriginal and Torres Strait Islander Flexible Aged Care Program (Australian Institute of Health and Welfare, 2023 Aged Care Provider Workforce Survey: Report, AIHW, Canberra, 2024).
Note b: The Aged Care Provider Workforce Survey 2026 opened on 16 February 2026 and ran for six weeks.
Source: DHDA, CHSP Program Manual 2025–27 (July 2025); and advice from DHDA to the ANAO in September 2025.
3.46 The ACQSC is responsible for reviewing CHSP providers against relevant Aged Care Quality Standards.95 Under the Aged Care Act 1997 and the ACQSC Act, the ACQSC does not have the power to revoke a CHSP provider’s authority to deliver services. The ACQSC can refer a provider to DHDA, which can respond to non-compliance by revoking the provider’s grant agreement. According to DHDA’s records, the ACQSC assessed 104 and 117 CHSP providers as non-compliant with the Aged Care Quality Standards in 2023–24 and 2024–25, respectively. DHDA has incomplete records on the outcome of the ACQSC’s assessments. DHDA advised the ANAO in November 2025 that ‘no revocations have been undertaken in this period as the CHSP was not governed under the previous Aged Care Act’.
3.47 In July 2021, DHDA began using an ‘escalated provider list’ (EPL) to identify and monitor provider non-compliance and underperformance. A provider is added to the EPL based on Community Grants Hub provider risk ratings; non-compliance with the Aged Care Quality Standards as determined by the ACQSC; escalations received from within DHDA (e.g. through the fraud section or state and territory offices); complaints; and media reports. DHDA has a CHSP compliance dashboard that identifies ‘providers of concern’, which DHDA advised the ANAO in November 2025 it has maintained since December 2024. The compliance dashboard identifies approximately 70 providers each month. DHDA advised the ANAO in September 2025 that the CHSP compliance dashboard is distributed to the Home Support Operations Board with meeting papers and discussed at meetings, as required. Nineteen of the 20 Board meeting packs for 2023–24 and 2024–25 reviewed by the ANAO did not include the compliance dashboard and for the one that did include it, it was incomplete. In August 2025, DHDA documentation stated that ‘on average, over the last two years, one in every three providers of concern were moved to a less serious status or opted to relinquish services because of the EPL process’. For 2024–25, the CHSP compliance dashboard states that providers relinquished a total of $12.4 million in grant funding. Appendix G of the CHSP Manual 2025–27 sets out the process and responsibilities for reallocating clients to ensure continuity of care following provider relinquishment.96
3.48 These assurance activities provide DHDA with some assurance over consistency with the service delivery principles established in the CHSP Manual. However, referrals from the Community Grants Hub and the ACQSC relate to the small population of providers that are identified as not doing the right thing. DHDA has no mechanisms to understand the quality of care that is being provided on a day-to-day basis by the vast majority of CHSP providers. Such assurance might be obtained through assurance activities identified in DHDA’s Assurance Framework, such as stakeholder engagement activities and surveys (including with participants and their carers), management-commissioned reviews and internal audits.
3.49 The CHSP Manual states that CHSP service delivery must consider the social, cultural, linguistic, religious, spiritual, psychological and medical care needs of all clients. The Older Persons Advocacy Network’s (OPAN) ‘presenting issues’ reports between 2020–21 and 2024–25 found that the provision of culturally appropriate care by aged care providers was an issue for diverse and vulnerable communities including Aboriginal and Torres Strait Islander Australians.97 Examples of the issues raised include consideration of a person’s dietary requirements, language barriers, people’s hesitation to use interpreter services, and care models assuming family support, housing stability, literacy and financial stability. The CHSP has no assurance mechanisms that go to the cultural appropriateness of service delivery. Results from the ANAO client survey relating to culturally safe care are described in Box 9 and suggest that a minority of CHSP clients have concerns relating to cultural safety.
|
Box 9: ANAO surveys — cultural safety |
|
Over half (57 per cent) of clients stated that aged care services provided in the last six months through the CHSP ‘definitely’ respected and understood their cultural or personal identity (25 per cent ‘somewhat’; 15 per cent ‘not really’ or ‘not at all’). In total, 351 survey respondents (two per cent) identified as being Aboriginal or Torres Strait Islander. Of these, 43 per cent said ‘definitely’ (27 per cent ‘somewhat’; 29 per cent ‘not really’ or ‘not at all’). Over half of all clients surveyed (58 per cent) stated that they were comfortable or very comfortable sharing their cultural or personal identity when receiving CHSP services (six per cent uncomfortable or very uncomfortable). Of First Nations clients, 12 per cent said they were uncomfortable or very uncomfortable. Between 24 per cent and 27 per cent of First Nations clients agreed or strongly agreed that services provided in the last six months through the CHSP supported their connection to family, kinship groups and country and ability to participate in culture practices or traditions (20 per cent disagreed or strongly disagreed). |
Recommendation no.7
3.50 The Department of Health, Disability and Ageing undertake risk-based assurance activities that provide confidence to decision makers that the Commonwealth Home Support Program is being managed within expectations and in accordance with legal and policy frameworks, including in relation to service delivery quality.
Department of Health, Disability and Ageing response: Agreed
3.51 The department will develop and implement a provider payments assurance framework for the CHSP, including through the commencement of provider focused assurance activities. This will enhance assurance over the appropriate use of funding and bring the department’s payments assurance arrangements for CHSP broadly into alignment with the approach in place for Support at Home. The department will seek Government consideration to implement risk-based assurance activities, including coverage of service delivery and quality risks, in the context of decisions on the future direction of CHSP and its transition to Support at Home.
Lessons learnt to support the transition to Support at Home
3.52 Documenting lessons learnt from the CHSP would support the effective transition of the CHSP to the Support at Home program. DHDA has identified lessons learnt for two CHSP activities: undertaking grant rounds; and the Q1 review process (paragraph 3.46). Other than these two examples, DHDA does not have a process for identifying or monitoring lessons learnt from CHSP activities, including to support the transition of the CHSP to the Support at Home program.
3.53 Under the MOU between the ACQSC and DHDA, the ACQSC is responsible for dealing with complaints it receives about a provider’s responsibilities under the Aged Care Act 1997 or funding agreement. The ACQSC shares trends in complaints it has received about the CHSP with DHDA through program assurance group (see paragraph 3.21). In 2024 and April 2025, the ACQSC publicly reported that the complaints themes for in home care included concerns about a lack of consultation, care coordination, fees and charges, and personal behaviour/conduct.98 There is no evidence that DHDA developed actions in response to the ACQSC complaints information.
3.54 DHDA may undertake enhanced monitoring and potential compliance action based on complaints regarding individual providers (see paragraph 3.46). DHDA has not consolidated the complaints information it receives to identify potential systemic program issues to inform a continuous improvement process.
Opportunity for improvement
3.55 DHDA could establish a process to consolidate and analyse participant complaints about the CHSP and a lessons learnt register to inform the transition to the Support at Home program.
4. Is the Commonwealth Home Support Program meeting its objectives?
Areas examined
This chapter examines whether the Commonwealth Home Support Program (CHSP) is meeting its objectives.
Conclusion
DHDA has not demonstrated, through performance reporting or evaluation, that the CHSP is meeting its objectives (which comprise, for clients: better quality of life, delaying admission to residential aged care, greater social connectivity, improved or maintained emotional and physical wellbeing, and greater independence). There is a public performance measure for the CHSP that reports on outputs and provides no information about the achievement of outcomes or program efficiency. DHDA monitors some performance data that is primarily related to grant agreement financial acquittals and outputs. DHDA has not evaluated the CHSP and has commissioned little research that supports an understanding of impact. ANAO research has found that the majority of stakeholders (CHSP providers, peak bodies and CHSP clients) believe that most objectives are being met, particularly improved quality of life.
Areas for improvement
The ANAO made two recommendations aimed at establishing outcomes-focused performance measures for the CHSP, and evaluating the extent to which CHSP objectives are being met to inform the CHSP’s transition to the new Support at Home program.
4.1 The object of the Aged Care Act 2024 includes promoting innovation and continuous improvement in the Commonwealth aged care system based on research.99
4.2 The Commonwealth Evaluation Policy aims to embed a culture of evaluation and learning from experience to underpin evidence-based policy and delivery. The policy is supported by the Department of the Treasury’s Resource Management Guide (RMG) 130 Evaluation in the Commonwealth (the Evaluation Toolkit). The Evaluation Toolkit states that putting in place planning arrangements for performance monitoring and evaluation support an evaluative culture.100 The Public Governance Performance and Accountability Act 2013 contains requirements for external performance reporting to promote accountability to ministers, the Parliament, and the public.101
4.3 DHDA established an Evaluation Strategy 2016–2019, which sets out DHDA’s approach to embedding a culture of evaluation to support robust evaluation of the department’s policies and programs. The Evaluation Strategy was updated in 2023. For projects, DHDA has a Project Management Framework that sets out expectations for the measurement and reporting of project benefits.
Is there fit-for-purpose performance measurement, monitoring and reporting?
There is a lack of performance measurement, monitoring and reporting of program quality, outcomes or efficiency. DHDA has one corporate plan performance measure for the CHSP that measures output (number of clients that access CHSP services). DHDA reported that it ‘substantially met’ the measure’s target of 840,000 CHSP clients in 2024–25. DHDA has established provider performance measures that relate to provider financial compliance with grant agreements. DHDA monitors the corporate plan performance measure, provider financial compliance and other program statistics on a monthly basis.
Performance measurement and reporting
4.4 Section 16EA of the Public Governance Performance and Accountability Rule 2014 (PGPA Rule) contains requirements for an Australian Government entity’s performance measures to be included in its portfolio budget statements, corporate plan and annual performance statements. The Department of Finance’s RMG 131 Developing performance information outlines principles to assist entities with meeting the PGPA Rule requirements.102 Performance measures should be relevant; reliable and verifiable; unbiased; contain a mix of qualitative and quantitative measures; contain a mix of output, efficiency, and effectiveness measures; and provide a basis for assessment over time.
4.5 DHDA has reported on CHSP in its annual reports since 2016–17.
- In 2015–16, DHDA established six corporate plan performance measures relating to the CHSP, which included ‘Number of people receiving CHSP services’ and ‘Number of CHSP older clients receiving services as a percentage of the target population’. In 2016–17, DHDA included three measures relating to the CHSP in its annual report, which included: ‘Number of older people receiving a service through the CHSP’.
- In 2017–18, DHDA had one measure for the CHSP in its annual report, which had a greater outcomes focus: ‘CHSP continues to assist older people to stay independent and live in their homes and communities for longer’. A similar measure was included in the 2018–19 and 2019–20 annual reports with minor wording variations. In 2020–21, there was no standalone measure for the CHSP, however the number of clients accessing the CHSP ‘to support independence and wellness at home’ was included as a target for the performance measure ‘Provide senior Australians with entry-level support to remain independent and live in their homes and communities for longer’.
- From 2021–22 to 2025–26, DHDA had one performance measure for the CHSP that was output-focused: ‘Number of clients that accessed CHSP services’.103 The performance measure target was 840,000 in 2024–25 and 860,000 in 2025–26.
4.6 For measures relating to the number of clients accessing CHSP services, DHDA ‘substantially met’ or ‘substantially achieved’ the target since 2016–17 (Figure 4.1).
Figure 4.1: Number of clients accessing CHSP services, 2016–17 and 2020–21 to 2024–25a
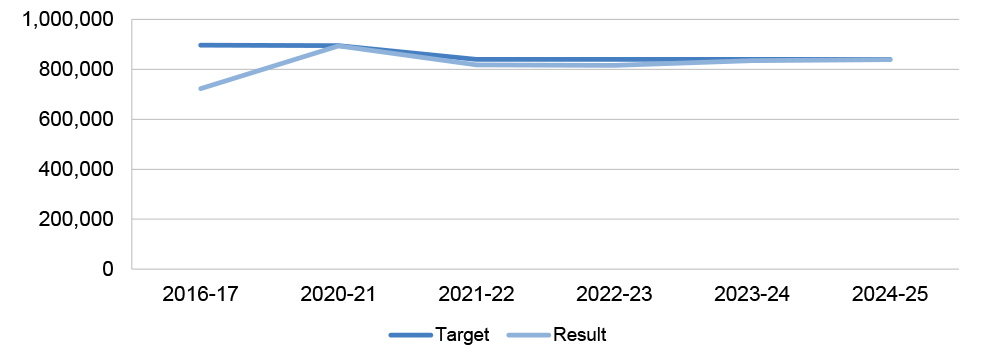
Note a: There were minor variations in performance measure wording between years.
Source: ANAO analysis of Department of Health, Disability and Ageing documentation.
4.7 Reporting on CHSP performance measures in 2017–18 to 2020–21 focused on outputs and provided no information about outcomes. The results stated: ‘Services were provided through the CHSP’ (described as ‘met’) or ‘Home support services were provided through the CHSP across all states and territories, with a focus on wellness and reablement’ (also described as ‘met’). There is no information in DHDA’s annual performance statements about whether the CHSP is achieving outcomes or is an efficient use of public funds.
4.8 The ANAO has concluded in its performance statements audits since 2022–23 that the annual performance statements for Programs 3.2 (Aged Care Services) and 3.3 (Aged Care Quality) under portfolio budget statements Outcome 3 (Ageing and Aged Care) were not considered a complete representation of all key functions of the programs.104
4.9 The ANAO has previously commented that for performance measures relating to Program 3.2 (Ageing and Aged Care), the ANAO was unable to determine if the results of performance measures were accurately reported, as the data was provided by external parties and had not been assured by DHDA (see paragraphs 2.20 and 3.37).105
4.10 The 2025–26 Corporate Plan states that new performance measures for the CHSP and the Support at Home program will be developed as part of the 2026–27 Federal Budget.106 DHDA advised the ANAO in April 2026 that new performance measures have not been developed and would be considered following a government decision on the future of the CHSP.
Recommendation no.8
4.11 The Department of Health, Disability and Ageing establish performance measures for the Commonwealth Home Support Program that facilitate monitoring of service delivery and public transparency over whether the program is efficiently meeting its objectives.
Department of Health, Disability and Ageing response: Agreed
4.12 The department will review the performance measures for CHSP to ensure they are fit for purpose and support clear monitoring of effective service delivery. Subject to ICT resourcing allocations and decisions of Government regarding the future direction and management of the CHSP, the department will establish performance measures that support public transparency and provide greater assurance as to whether the program is efficiently meeting its objectives.
4.13 DHDA has provided no other advice to government about the performance and effectiveness of the CHSP.
Performance monitoring
4.14 DHDA has grant agreement performance measures relating to provider compliance with agreement requirements. Measures comprise the number of units of a service delivered in the financial year (e.g. the number of hours of the service provided) and the funding expended by the provider against a target (which is set out in an activity work plan and determined by grant funding provided). This is aggregated across all providers to the service type and national level against service type and national targets. The Home Support Operations Branch monitors the corporate plan performance measure (number of clients accessing CHSP services), delivery of outputs, and other program-level statistics. From February 2024, performance information was monitored through a monthly data dashboard (see paragraph 2.10). The dashboard tracks year to date and in comparison to the same month in the previous year:
- total number of delivered outputs (114,535,386 in 2024–25);
- total number of funded providers (1,273);
- total number of CHSP clients (838,694) and the number of CHSP clients who are male (296,940) and female (531,715) and neither (10,039)107, culturally and linguistically diverse (168,376) and of Aboriginal or Torres Strait Islander status (23,894);
- total number of CHSP referrals and recommendations (4,797,018) and the number of CHSP clients with a CHSP referral (549,251);
- total client contributions ($329,268,098) and average funding provided per client ($3,927);
- number of providers due to relinquish CHSP services (16); and
- ‘overall performance’, which is defined as the proportion of targeted ‘outputs’ that are delivered (83 per cent as at 30 June 2025) and performance by each service type (ranging from 62 per cent for other food services to 96 per cent for goods, equipment and assistive technology).
4.15 Expenditure against funding allocations is also monitored by the Home Support Operations Branch at the national level (see paragraph 2.10) through the data dashboard.
4.16 DHDA reviews and reports on performance reporting documents and processes to the Audit and Risk Committee twice annually.
Is there fit-for-purpose evaluation?
Other than planning for an evaluation of one CHSP project, DHDA has not planned to evaluate the CHSP against its objectives and has not evaluated the appropriateness of CHSP funding arrangements and key policy settings. DHDA has conducted or commissioned reviews of some components of the CHSP. DHDA cannot demonstrate the CHSP is meeting the program’s objectives.
Evaluation planning
4.17 DHDA’s 2023–2026 Evaluation Strategy states that divisions must ensure all new and existing policies and programs have a monitoring and evaluation framework and establishes three evaluation tiers to prioritise evaluation effort and resourcing. Tier 1 policies or programs have high strategic importance, funding, risk and impact, and lack a current evidence base. The evaluation of tier 1 policies or programs may be characterised by extensive consultation, high evaluation resource allocation, high quantitative data requirements, comprehensive qualitative information and comprehensive evaluation reports.
4.18 DHDA has not categorised the CHSP using the tiering system despite its size and scope (annual funding exceeding $3 billion, supporting almost 840,000 people) and its inclusion as a key activity under the Aged Care Services program in the DHDA’s Portfolio Budget Statements.
4.19 DHDA’s 2023–2026 Evaluation Strategy states that an evaluation schedule would be developed for higher priority policies and programs. In September 2024, DHDA established an evaluation schedule, which was updated in July 2025, that documents the status of planned, in progress and completed evaluations. An evaluation of the CHSP was not listed.108
4.20 DHDA’s Project Management Framework states that all projects are implemented with an expectation they will result in benefits; all projects will identify and put in place measurement of expected benefits; and benefits management activities will be proportional to the size and importance of the expected benefit. A tier 1 project is defined as having a budget over $10 million, being of higher complexity and a priority of government, carrying reputational risk and having a high number of stakeholders. Tiering allows the project management approach, which includes benefits management and measurement, to be ‘scaled to reflect the project’s risk profile and strategic importance’.
4.21 The 2024–25 CHSP grant extension project (see paragraph 3.31) was identified as a tier one project in August 2023. This project has not been evaluated and no evaluation is planned. In July 2025, DHDA’s Aged Care Governance Committee (paragraph 3.18) considered a list of planned and commenced aged care project evaluations, including for two projects related to CHSP: the GEAT2GO CHSP pilot delivery model109 (planned for late 2025); and 2024 CHSP grant funding rounds (planned for early 2026). DHDA advised the ANAO in September 2025 that an evaluation is planned for the tier 1 2025–2027 CHSP extension project.
4.22 To support evaluation, a program logic model is a useful tool to show how a program is intended to work; establish the connection between resources, activities and intended outcomes; and identify measures of success.110 DHDA’s 2023–2026 Evaluation Strategy states that divisions must ensure all new and existing policies and programs have a program logic. DHDA has developed program logics at the portfolio budget statements program (see Appendix 8) and project level that are relevant to the CHSP, although the program logics for the portfolio budget statements program and the CHSP were developed late in the programs’ life cycles. For example, in 2023, eight years after the program’s establishment, DHDA commissioned Callida Consulting to develop a program logic for the CHSP.111 In 2025, DHDA established a program logic model for the broader Program 3.2 (Aged Care Services), which describes programs such as the CHSP, residential aged care and the Support at Home program as outputs leading to short (direct program attribution), medium (behavioural change) and long-term (system change) outcomes. The long-term outcomes are described as:
An aged care system that places older people and their rights at the centre, to support their ability to live active, self-determined and meaningful lives. Older people receive care and support at home or in residential care that contributes to their autonomy, independence and quality of life.
4.23 In 2023, DHDA engaged Health Policy Analysis to develop an evaluation strategy for the new Support at Home program to improve the design of the program and its implementation.112 A draft strategy was developed in May 2023 that states a finalised version will be established in June 2023. The draft strategy included a program logic, evaluation questions, methods and data sources. The strategy has not been finalised.
Evaluation activities
4.24 Between 2019–20 to 1 November 2025, DHDA has conducted or commissioned reviews of some components of the CHSP, including:
- between February 2019 and December 2020, Australian Healthcare Associates conducted an evaluation of the Better Ageing: Promoting Independent Living (PIL) Federal Budget measure113;
- in 2020, Deloitte conducted data analysis to understand variation in CHSP service cost and type between different client demographics114;
- in 2021, ACIL Allen conducted a review of CHSP service costs, with the aim of developing an appropriate funding and pricing policy for the CHSP115;
- in April 2023, Callida Consulting did a desktop ‘long form review’ of the CHSP to capture status updates of performance and evaluation activities, stakeholder engagement, data, compliance, risks, and issues for reporting to DHDA’s Program Assurance Committee116; and
- in November 2024, DHDA completed an evaluation of the 2024–25 CHSP growth round project (see paragraph 2.6).
4.25 The Callida Consulting long form review was finalised in October 2023 and proposed three actions to which DHDA agreed and assigned an action owner:
- improving data analysis and monitoring through dashboards that integrate all data sources (provider data management systems, My Aged Care and the provider Data Exchange (DEX));
- increasing provider compliance management activity; and
- setting clear and specific objectives for the CHSP, with an emphasis on the centrality of client outcomes, choice and control.
4.26 Since the CHSP was established in 2015, DHDA has not undertaken a comprehensive program evaluation examining CHSP policy settings and whether the program is meeting objectives. In advice to the Minister for Aged Care supporting proposed spending on First Nations growth funds in 2023 (see Table 2.1), DHDA stated: ‘An evaluation of the CHSP was effectively undertaken in 2018 as part of the Royal Commission into Aged Care Quality and Safety [Royal Commission].’ The Royal Commission did not evaluate the CHSP and the CHSP was not the Royal Commission’s focus.117
4.27 In 2023, the Australian Public Service Commission published a Capability Review of DHDA. The review noted that, although there were pockets of good evaluation in DHDA, DHDA’s evaluation function was ‘developing’; it lacked an evaluation culture; evaluations had been outsourced; not included in policy and program design at inception, or done after the event to meet evaluation requirements; and responsibility for evaluation was devolved to program areas that lacked capability. The review gave grant programs as one example of where DHDA could improve given DHDA is the single largest granting agency in the Commonwealth, and commented on DHDA feedback about ‘the difficulty in evaluating grants and having ownership of the outcomes when not involved in all stages of the grant’. The review noted work that DHDA was undertaking at the time to improve evaluation, such as receiving ongoing funding for evaluation in the 2023–24 Federal Budget, updating the Evaluation Strategy, and launching a new Evaluation intranet site with resources.118
Is the Commonwealth Home Support Program meeting objectives?
There is little available research that examines the impact of the CHSP or the extent to which the CHSP’s objectives are being met. Available data on the impact of in home aged care services more generally indicates a downward trend in the use of residential aged care (a CHSP objective), however there is a lack of longitudinal data that would help establish causality. ANAO research suggests that a majority of stakeholders (CHSP clients, aged care peak bodies and CHSP providers) believe that most objectives are being met. The proportion of CHSP clients that reported a little or a lot of improvement in outcomes ranged from 32 per cent (ability to participate in your community) to 66 per cent (quality of life). First Nations clients were less likely than average to report improved outcomes.
4.28 The CHSP Manual 2025–27 states that the program has five objectives. The CHSP supports older people who are having difficulties with daily living to:
- have a better quality of life;
- continue living in their own homes, and/or delay admission to residential care;
- participate more in their community and have more face-to-face and online social connections;
- maintain and/or improve their psychological, emotional and physical wellbeing; and
- be more independent at home and in the community.
4.29 There has been limited research into the CHSP’s achievement of these objectives.
- The final report of the Royal Commission recommended the development of a comprehensive suite of quality indicators for people receiving aged care in residential care and at home. In October 2021, Flinders University prepared a report for DHDA that provided a comprehensive evidence review of validated tools to measure quality of life and consumer experience of and satisfaction with aged care. The report examined the tools’ appropriateness for residential aged care and home care settings for the purposes of incorporation into Australia’s National Aged Care Mandatory Quality Indicator Program (QI Program).119 The report identified a total of 12 quality of life tools that had been applied across Australia in home care settings.
- Research conducted by the Australian Institute of Health and Welfare (AIHW) on mental health in aged care was not specific to the CHSP. In July 2024, the AIHW reported on mental health in aged care using data collected between 1 July 2017 and 30 June 2022. The data captured mental health needs at the time of assessment for aged care services. On average, 23 per cent of all people aged 65 years and over that started receiving a Home Care Package were recorded to have a mental health condition.120 This proportion was higher than the reported prevalence of mental health conditions in the general population of older adults (7.9 per cent of men and 11.1 per cent of women aged 65 to 85 years). There is no assessment of mental health condition after entry to aged care services generally or of the CHSP specifically. It is therefore unknown if CHSP supports maintenance or improvement in the psychological and emotional wellbeing of older people.
- In terms of delaying admission to residential aged care, in April 2025 the AIHW reported on the number of people using aged care services (the CHSP, Home Care Packages Program and residential care), including trends over time from 1 July 2017 to 30 June 2024. After accounting for growth in the older population, the data demonstrates that between 2017 and 2024: the number of people aged 65 years and older using permanent residential care decreased by 11 per cent; using the Home Care Packages Program more than tripled; and using the CHSP decreased by 4.2 per cent. There is a slight negative correlation between CHSP participation and use of residential aged care. As this research was not longitudinal and did not seek to establish causality between receiving home care and requiring residential care, it is not helpful in establishing whether the CHSP is achieving its objective of delaying admission to residential aged care.
- DHDA has not conducted, commissioned or used any research that examines the impact of the CHSP on social connectivity or client independence.
Recommendation no.9
4.30 The Department of Health, Disability and Ageing establish an evaluation plan for the Commonwealth Home Support Program and evaluate the extent to which the Commonwealth Home Support Program objectives are being met, to inform the Commonwealth Home Support Program’s transition to the Support at Home program.
Department of Health, Disability and Ageing response: Agreed
4.31 The department will establish an evaluation plan for the CHSP and undertake an evaluation to assess the extent to which the program is achieving its objectives. The scope, timing and focus of the evaluation plan, and the conduct of an evaluation, will be informed by any decisions of government on future arrangements for the CHSP.
4.32 In September 2025, the ANAO invited 1,486 employees of 1,168 CHSP providers and 19 peak bodies to provide feedback on the CHSP through an online survey (see Appendix 4 and Appendix 5). In total, 495 people from 436 provider organisations (33 per cent response rate) and representatives of nine peak bodies (47 per cent response rate) completed the surveys. In November to December 2025, the ANAO invited 159,997 CHSP clients to provide feedback on the CHSP through an online survey (see Appendix 6). In total, 10,125 clients completed the survey (6.5 per cent response rate). Box 10 shows results from survey questions exploring the extent to which CHSP objectives are being met, which indicate that stakeholders generally believe the CHSP to be meeting its objectives.
|
Box 10: ANAO surveys — Achievement of program objectives |
|
In relation to whether DHDA collects the right information to determine if the CHSP is meeting its objectives, ANAO surveys found (see Appendix 4 and Appendix 5):
Four in nine peak bodies and 80 per cent of providers agreed or strongly agreed that the services available through the CHSP are appropriate to meet the program objectives. The majority of providers and peak bodies agreed or strongly agreed that the CHSP is achieving its objectives.
Based on the aged care services they had received in their home from a local provider through the CHSP in the last six months, clients reported a little or a lot of improvement in (see Appendix 6):
Among clients:
|
Note a: Independence is understood to mean the ability to perform daily personal and domestic tasks and make decisions about health and lifestyle.
Australian Institute of Family Studies, Social isolation: Factors, dynamics and effects of isolation for older people [Internet], AIFS, Melbourne, 2024, available from https://aifs.gov.au/research/research-snapshots/social-isolation-factors-dynamics-and-effects-isolation-older-people [accessed 3 October 2025]
Department of Health Victoria, Independence [Internet], Department of Health Victoria, Melbourne, 2016, available from https://www.health.vic.gov.au/dementia-friendly-environments/independence [accessed 3 October 2025]
Aged Care Research and Industry Innovation Australia, Functional Independence [Internet], ARIIA, Tonsley, 2024, available from https://www.ariia.org.au/knowledge-implementation-hub/rehabilitation-reablement-and-restorative-care/rehabilitation-care-evidence-themes/functional-independence [accessed 5 November 2025].
Appendices
Appendix 1 Department of Health, Disability and Ageing response
Appendix 2 Improvements observed by the ANAO
1. The existence of independent external audit, and the accompanying potential for scrutiny improves performance. Improvements in administrative and management practices usually occur: in anticipation of ANAO audit activity; during an audit engagement; as interim findings are made; and/or after the audit has been completed and formal findings are communicated.
2. The Joint Committee of Public Accounts and Audit (JCPAA) has encouraged the ANAO to consider ways in which the ANAO could capture and describe some of these impacts. The ANAO’s corporate plan states that the ANAO’s annual performance statements will provide a narrative that will consider, amongst other matters, analysis of key improvements made by entities during a performance audit process based on information included in tabled performance audit reports.
3. Performance audits involve close engagement between the ANAO and the audited entity as well as other stakeholders involved in the program or activity being audited. Throughout the audit engagement, the ANAO outlines to the entity the preliminary audit findings, conclusions and potential audit recommendations. This ensures that final recommendations are appropriately targeted and encourages entities to take early remedial action on any identified matters during the course of an audit. Remedial actions entities may take during the audit include:
- strengthening governance arrangements;
- introducing or revising policies, strategies, guidelines or administrative processes; and
- initiating reviews or investigations.
4. In this context, the below actions were observed by the ANAO during the course of the audit. It is not clear whether these actions and/or the timing of these actions were planned in response to proposed or actual audit activity. The ANAO has not sought to obtain assurance over the source of these actions or whether they have been appropriately implemented.
- In May 2025, the Department of Health, Disability and Ageing (DHDA) established ‘Aged Care Service Demand Projection’ guidance ‘to describe the methodology (assumptions and calculations) for calculating future demand for aged care services by service type’ (paragraph 2.29).
- In June 2025 and November 2025, DHDA updated the Commonwealth Home Support Program Manual 2025–27 (paragraph 2.2).
- In June 2025, November 2025, and March 2026 DHDA updated the My Aged Care Assessment Manual (Version 8.1) (paragraph 2.42).
- In July 2025, DHDA updated and released the Commonwealth Home Support Program (CHSP) service catalogue 2025–27 (paragraph 1.6)
- In July 2025, DHDA commenced monthly meetings with Ageing Australia about the Commonwealth Home Support Program (CHSP) (paragraph 3.10).
- In July 2025, DHDA updated the terms of reference for the Home Support Operations project board (paragraph 3.18).
- In August 2025, DHDA established a ‘performance monitor tracker’ that monitors providers’ reported delivery against their contracted activities (paragraph 3.40).
- In August 2025, the Aged Care Governance Committee received a paper proposing options for new demand modelling to meet a range of different purposes for the Commonwealth Home Support Program, including the ‘Identification of regions with high growth in demand and/or demand which exceeds supply’ (paragraph 2.29).
- In September 2025, DHDA developed a program logic for the GEAT2GO pilot program (paragraph 4.19) after the program was implemented. DHDA developed draft evaluation questions and a data matrix to support an evaluation of the project.
- The 2025–26 Corporate Plan states that new performance measures for the CHSP and the Support at Home program will be developed as part of the 2026–27 Federal Budget (paragraph 4.10).The March 2026 Aged Care Assessment Manual includes key performance indicators for assessment providers that align with annual report targets on assessment timeliness. These will be enforceable from 1 July 2026. (see paragraph 2.52)
Appendix 3 Commonwealth Home Support Program timeline of activities
1. The Commonwealth Home Support Program (CHSP) was announced in April 2012 as an entry-level in home aged care program that operates alongside the Home Care Packages (HCP) Program and Short-Term Restorative Care Program (STRC), which are both intended for people with higher support needs than the CHSP is intended to support.
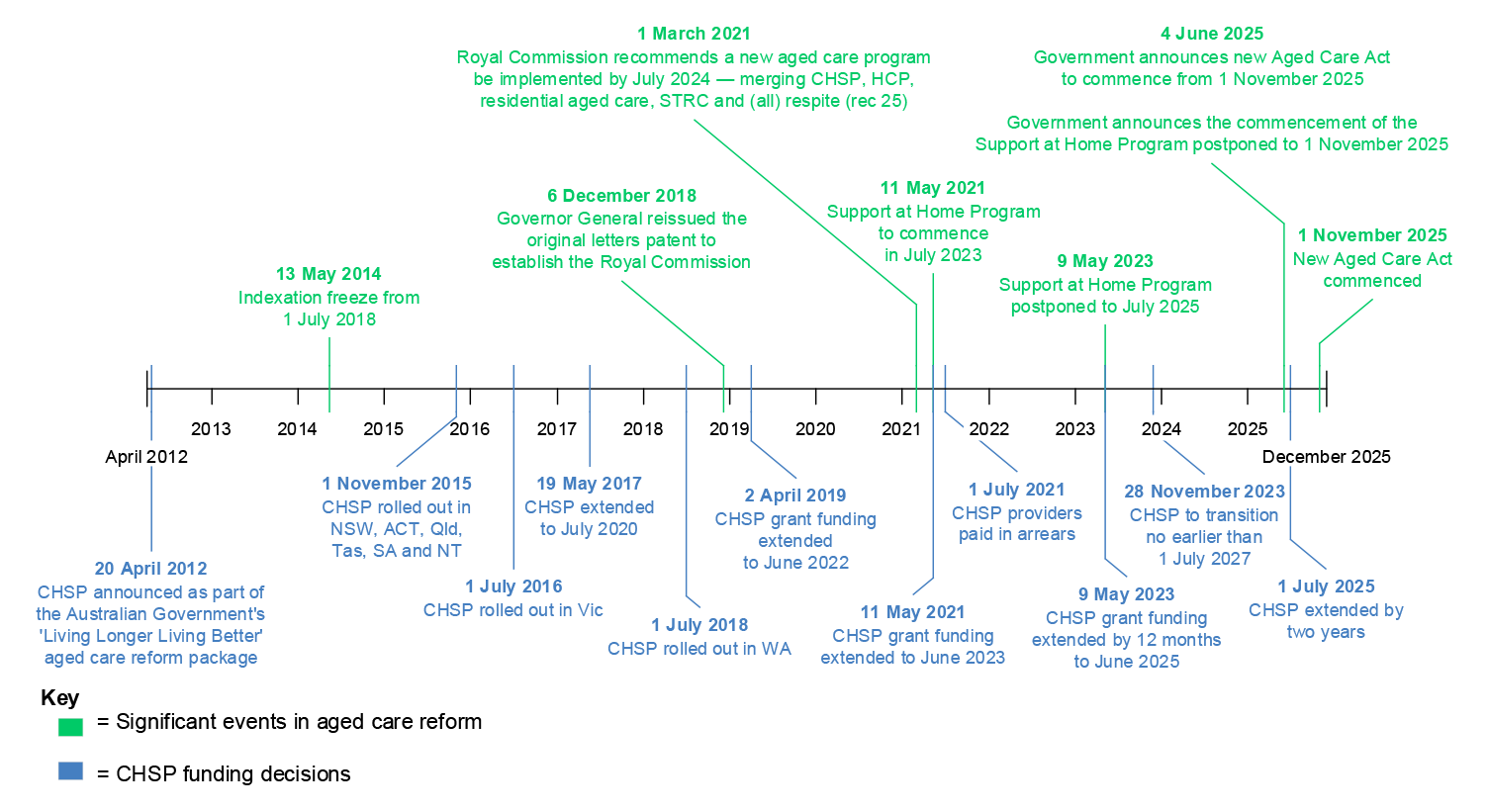
Appendix 4 Commonwealth Home Support Program provider survey
1. The audit undertook an online survey of Commonwealth Home Support Program (CHSP) providers. Two CHSP providers (Melton City Council and Carers and Disability Link) assisted the ANAO with finalisation of survey questions.
2. The Department of Health, Disability and Ageing (DHDA) provided the ANAO with a list of all 2024–25 CHSP providers, which comprised 1,718 employees of 1,243 providers.
3. The contact details for 75 providers and 200 employees were incorrect; in instances where there was no other contact in the original distribution list and an out-of-office reply identified an alternative contact, the ANAO emailed the nominated contact with a survey invitation. The ANAO sent a survey invitation to 1,486 employees from 1,168 provider organisations.
4. The survey was conducted between 10 September and 26 October 2025.
5. A total of 495 responses were received (response rate 33 per cent). The ANAO provided an option for people to provide anonymous responses. Ninety-eight per cent of respondents identified their organisation, representing 436 providers.121
6. Figure A.1 to Figure A.5 provide the survey results for the quantitative questions asked in the survey.
Figure A.1: Provider views on: Meeting community need
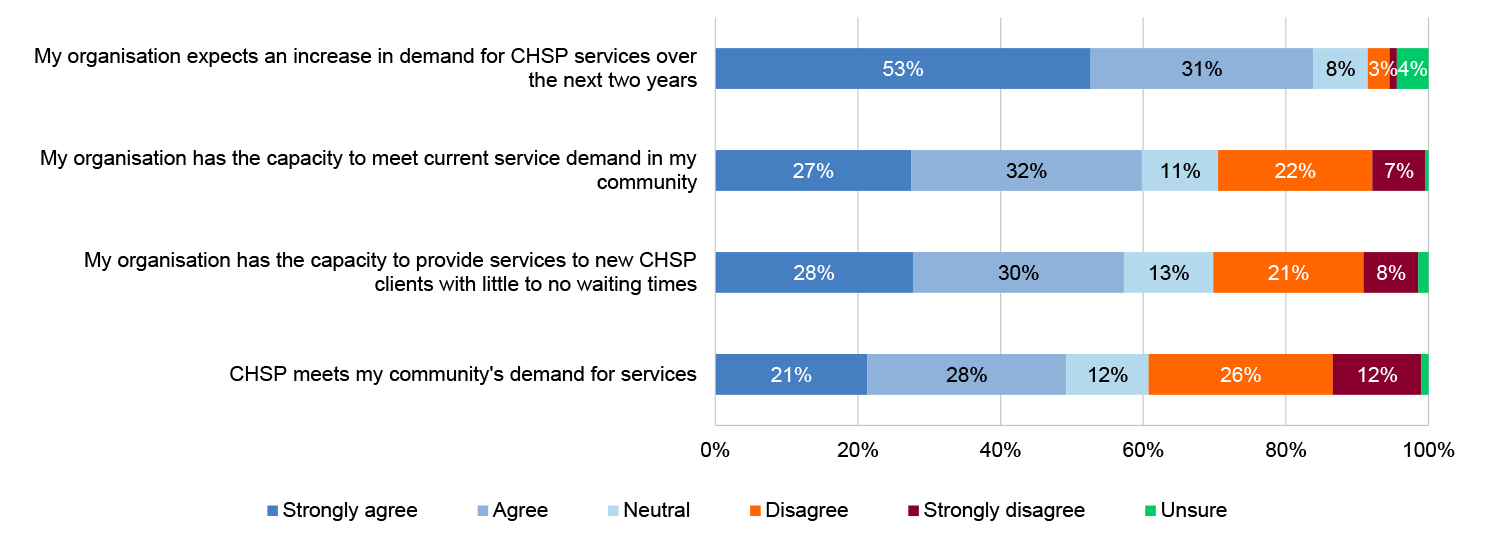
Source: ANAO provider survey.
Figure A.2: Provider views on: Effective service delivery
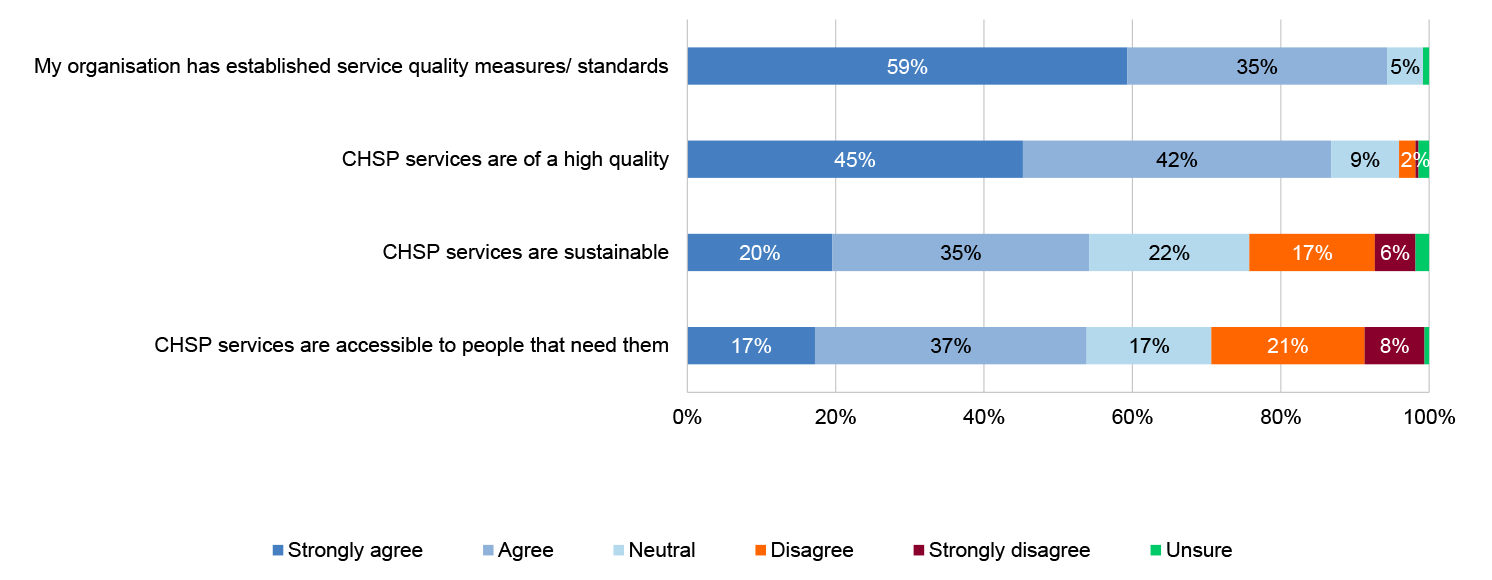
Source: ANAO provider survey.
Figure A.3: Provider views on: Meeting CHSP objectives
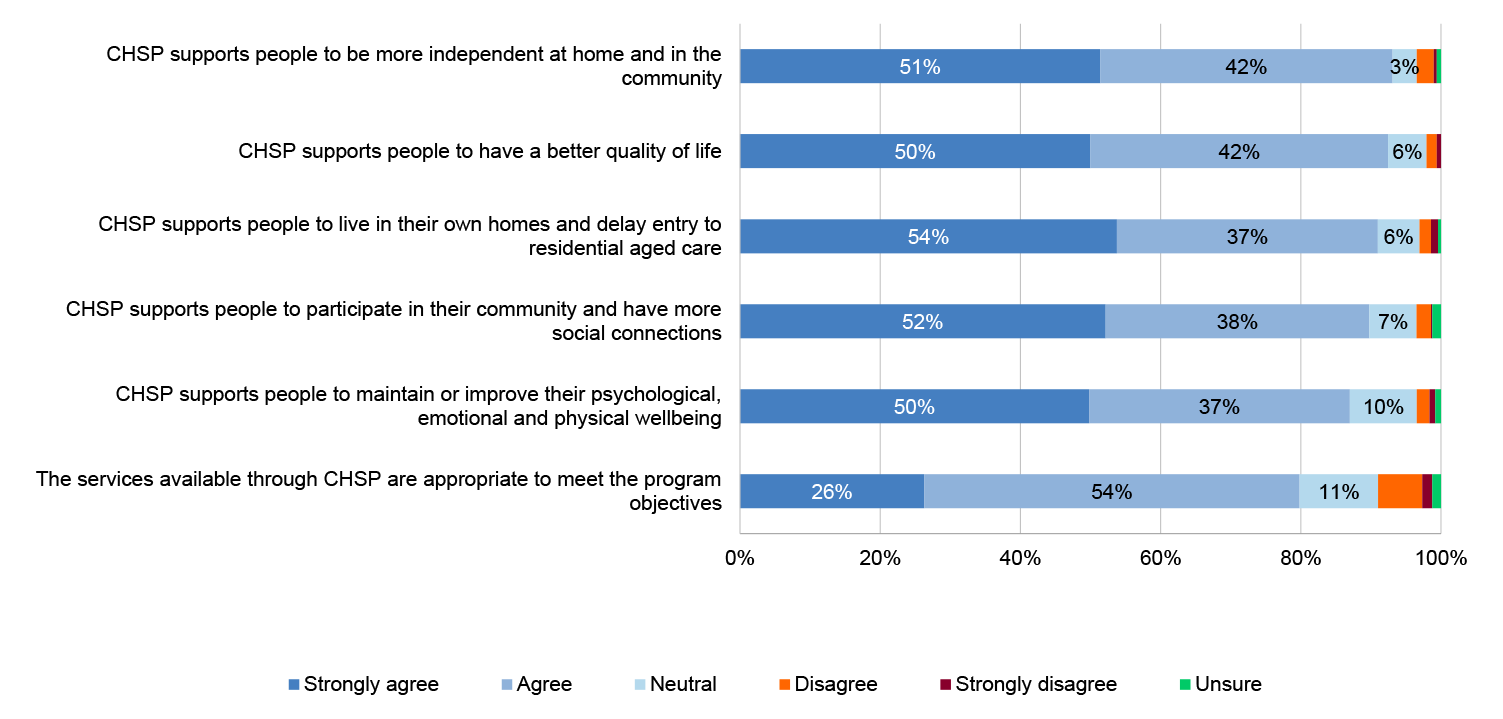
Source: ANAO provider survey.
Figure A.4: Provider views on: engagement with providers
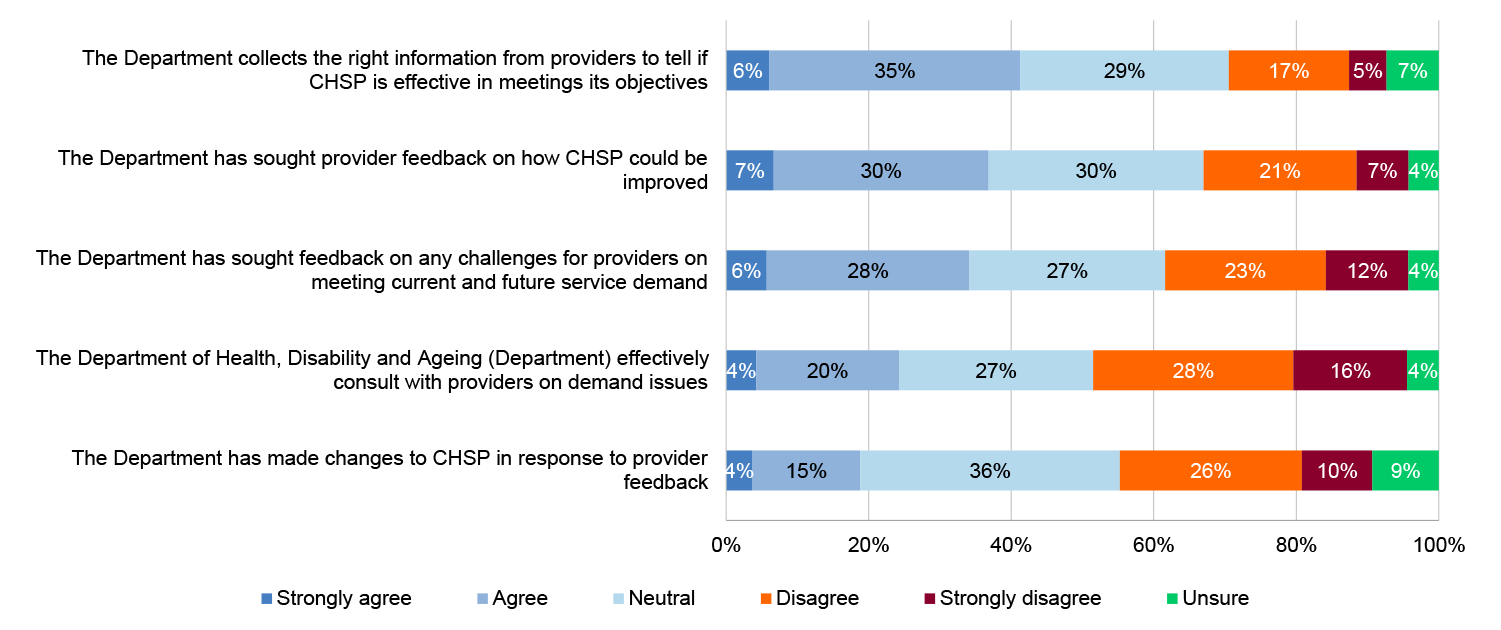
Source: ANAO provider survey.
The survey included eight free text questions. The key themes identified through analysis of the free text responses are outlined in Table A.1, with the frequency of the themes illustrated in Table A.2.
Table A.1: Key themes from Commonwealth Home Support Program provider survey
|
Themes |
Key points identified |
|
Access and assessment |
CHSP clients face barriers to accessing CHSP services, with the My Aged Care portal and assessment process described as confusing and administratively burdensome. Wait times for assessments mean some clients can wait many months for support, during which their needs worsen. These challenges hit CALD communities and people with low digital literacy hardest, exacerbating existing inequities. |
|
Communication |
Providers identified challenges with existing communication and engagement with the Department of Health, Disability and Ageing (DHDA), with the need for more consistent and timely information on policy changes, reporting requirements and funding allocations to support providers to plan and respond effectively. Providers reported that they would like opportunities to engage with DHDA in two-way communication. Providers identified the importance of the Funding Arrangement Manager (FAM) [within the Community Grants Hub] and the opportunity for regular engagement with the FAM can support and supplement information received through DHDA webinars and surveys. |
|
Compliance and administrative burden |
Providers report an increased compliance and reporting burden for the CHSP that is expensive and time consuming and diverts resources away from delivering services. Providers identified issues with the referral process through My Aged Care, creating an administrative burden for staff and delays to service delivery for perspective clients. Providers suggest that streamlined compliance and reporting requirements would decrease administration and improve their capacity to deliver client care. |
|
Cultural |
Gaps exist in services like allied health, home maintenance, and transport, especially in rural and remote areas where one provider might cover several communities across large distances. For Aboriginal and Torres Strait Islander and culturally and linguistically diverse (CALD) communities, cultural and language barriers make it harder to access CHSP services. |
|
Demand and capacity |
Funding shortfalls and workforce constraints impact on providers’ ability to meet rising demand and increasingly complex client needs. These pressures are most severe in rural and remote areas where thin markets and isolation magnify funding pressures and workforce issues. This results in waitlists, closed portals, and clients being turned away or forced to seek private alternatives. |
|
Funding |
Funding has not kept pace with increasing demand, population growth, demographic changes, and growing complexity of client needs, creating resource constraints across all states and most service types. These challenges are most pronounced in rural and remote areas, where thin markets and geographic isolation exacerbate service gaps. |
|
Program design and transition |
Providers are concerned about the transition to the Support at Home program, citing concerns over losing block funding, increased administrative burden, and reduced flexibility. There is particular anxiety in thin markets in rural and remote regions where providers warn of service withdrawal and possible market failure. |
|
Quality |
Providers report that existing reporting and compliance processes are burdensome with limited evidence that these requirements improve services and outcomes for older people. Providers raise concerns about the challenges of recruiting suitable staff in rural and remote areas and about the adequacy of funding to delivery high quality care. These challenges impact and divert resources away from care and support for older people. |
|
System |
Providers report difficulties in navigating IT systems, describing the Data Exchange (DEX) and the My Aged Care portal as clunky and difficult to navigate. |
|
Wellbeing and connectedness |
Delays or service delivery gaps have a human cost, leading to social isolation, hospitalisation, carer stress, burnout, and heightened mental health risks. These impacts are most severe in rural and remote areas, where geographic isolation and workforce shortages leave people with few alternatives when CHSP services are not available. The result is diminished wellbeing and independence, as vulnerable clients lose social connection and support networks. |
|
Workforce |
Recruitment and retention of qualified staff are barriers to timely access to CHSP services. This is compounded by low pay, high travel costs, and limited accommodation options in rural and remote communities. |
Source: ANAO provider survey.
Table A.2: Key themes heatmap
|
Question |
Themes |
||||||||||
|
|
Access and assessment |
Communication |
Compliance and administration burden |
Cultural |
Demand and capacity |
Funding |
Program design and transition concerns |
Quality |
System |
Wellbeing and connectedness |
Workforce |
|
Please provide any further feedback on CHSP meeting community need |
|||||||||||
|
Are there any specific issues or challenges your organisation experiences that impacts your ability to effectively deliver CHSP services |
|||||||||||
|
Please provide any further feedback on effective service delivery |
|||||||||||
|
Please provide any further feedback on CHSP meeting its objectives |
|||||||||||
|
Do you have any additional feedback on how the Department works with providers to: support effective delivery of CHSP services; and meet the CHSP objectives |
|||||||||||
|
Please provide any additional feedback you would like to provide to the ANAO |
|||||||||||
Key:
Low frequency
Medium frequency
High frequency
Source: ANAO provider survey.
7. Survey respondents were asked three questions about the type of service and location with survey results shown in Table A.3 and Table A.4.
Table A.3: Services provided by the respondents’ organisations
|
Service categories |
Responsesa |
Percentage (%) |
|
Allied health and therapy services |
139 |
28 |
|
Community cottage respite |
37 |
7 |
|
Domestic assistance |
223 |
45 |
|
Equipment and products |
39 |
8 |
|
Hoarding and squalor assistance |
13 |
3 |
|
Home adjustments |
77 |
16 |
|
Home maintenance and repairs |
189 |
38 |
|
Home or community general respite |
170 |
34 |
|
Meals |
220 |
44 |
|
Nursing care |
87 |
18 |
|
Person care |
166 |
34 |
|
Sector support and development |
59 |
12 |
|
Social support and community engagement |
343 |
69 |
|
Specialised support services |
47 |
9 |
|
Therapeutic services for independent living |
25 |
5 |
|
Transport |
232 |
47 |
Note a: Respondents were able to select multiple services.
Source: ANAO provider survey
Table A.4: Service delivery locations
|
Location |
Responsesa |
Percentage (%) |
|
State and territory |
||
|
Australian Capital Territory |
22 |
4 |
|
New South Wales |
159 |
32 |
|
Northern Territory |
16 |
3 |
|
Queensland |
139 |
28 |
|
South Australia |
58 |
12 |
|
Tasmania |
31 |
6 |
|
Victoria |
121 |
24 |
|
Western Australia |
38 |
8 |
|
Modified Monash (MM) area |
||
|
MM1 (metropolitan areas) |
248 |
50 |
|
MM2 (regional centres) |
143 |
29 |
|
MM3 (large rural towns) |
108 |
22 |
|
MM4 (medium rural towns) |
132 |
27 |
|
MM5 (small rural towns) |
172 |
35 |
|
MM6 (remote communities) |
65 |
13 |
|
MM7 (very remote communities) |
48 |
10 |
Note a: Respondents were able to select multiple locations.
Source: ANAO provider survey
Appendix 5 Aged care peak body survey
1. The audit undertook an online survey of aged care peak bodies asking questions about peak bodies’ views of the Commonwealth Home Support Program (CHSP) and engagement with the Department of Health, Disability and Ageing (DHDA).
2. The ANAO sent out a survey invitation to 19 organisations. The survey ran from 8 to 30 September 2025. Nine responses were received (47 per cent response rate) (Table A.5).
Table A.5: Commonwealth Home Support Program peak body respondents
|
Organisation type |
Number of respondentsa |
|
Represents the views of older people and/or their carers and representatives |
6 |
|
Represents the views of aged care providers |
4 |
|
Provides aged care services |
1 |
Note a: Peak bodies were able to select multiple responses.
Source: ANAO CHSP peak body survey.
3. The following figures provide the survey results for the quantitative questions asked in the survey.
Figure A.5: Aged care peak body views on: effectiveness of the Commonwealth Home Support Program
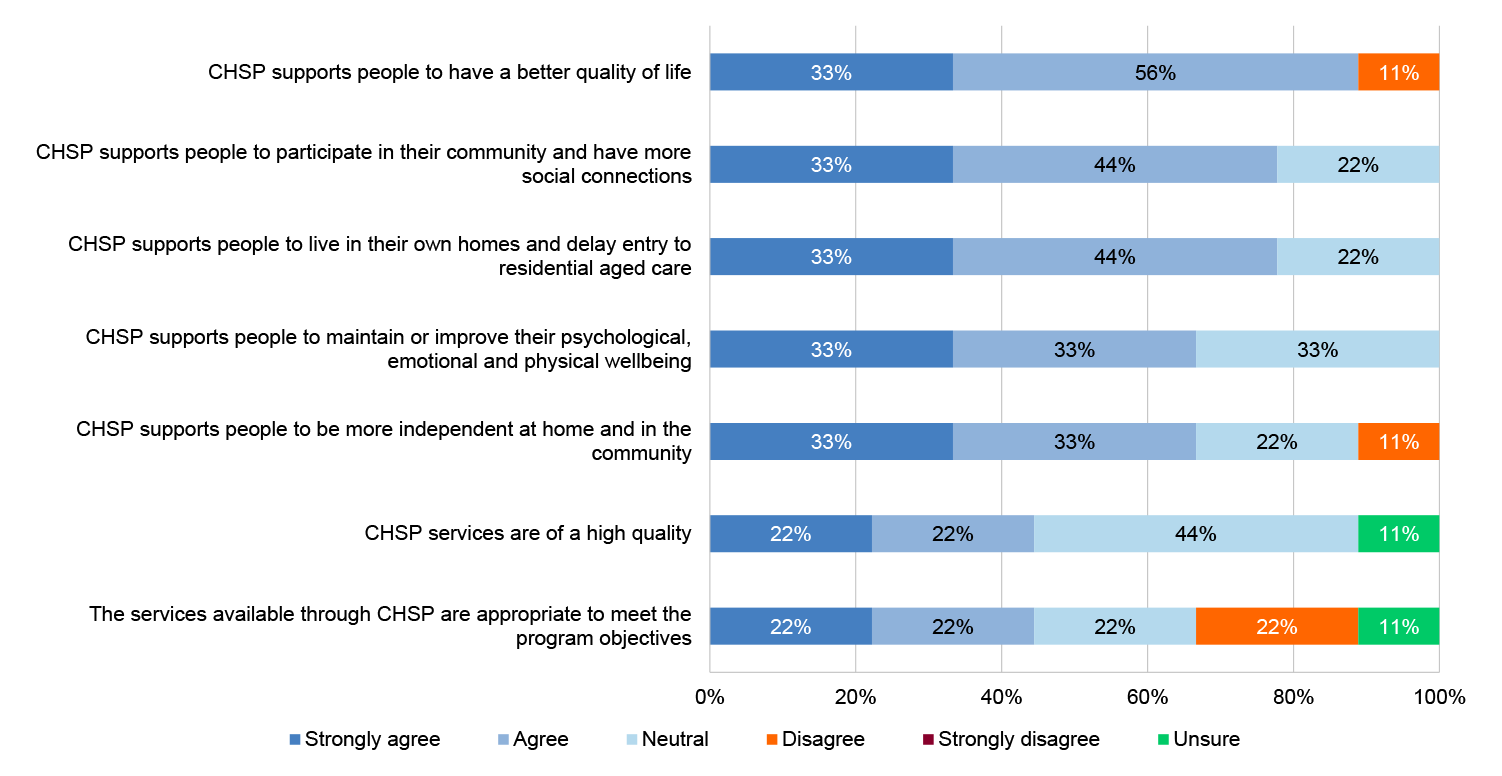
Source: ANAO peak body survey.
Figure A.6: Aged care peak body views on: Supply of and demand for the Commonwealth Home Support Program
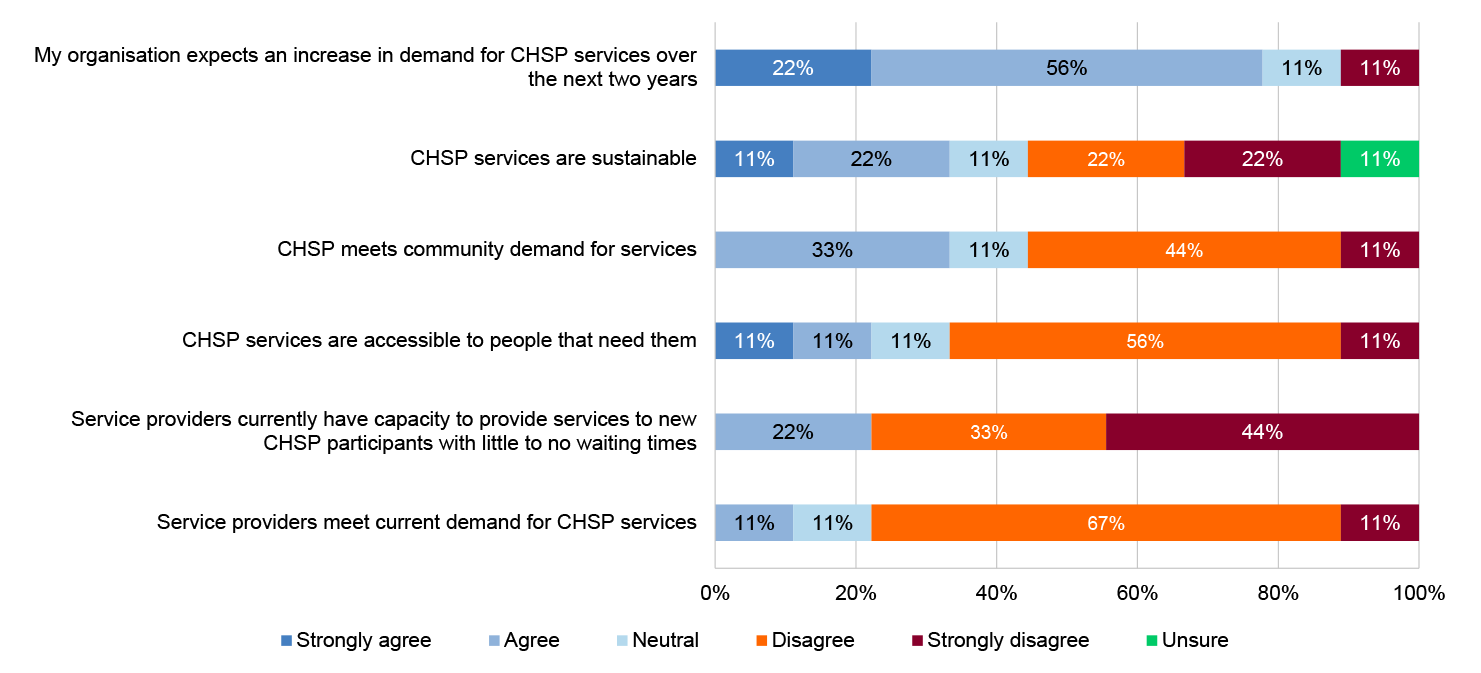
Source: ANAO peak body survey.
Figure A.7: Peak body views on: Department of Health, Disability and Ageing engagement with stakeholders
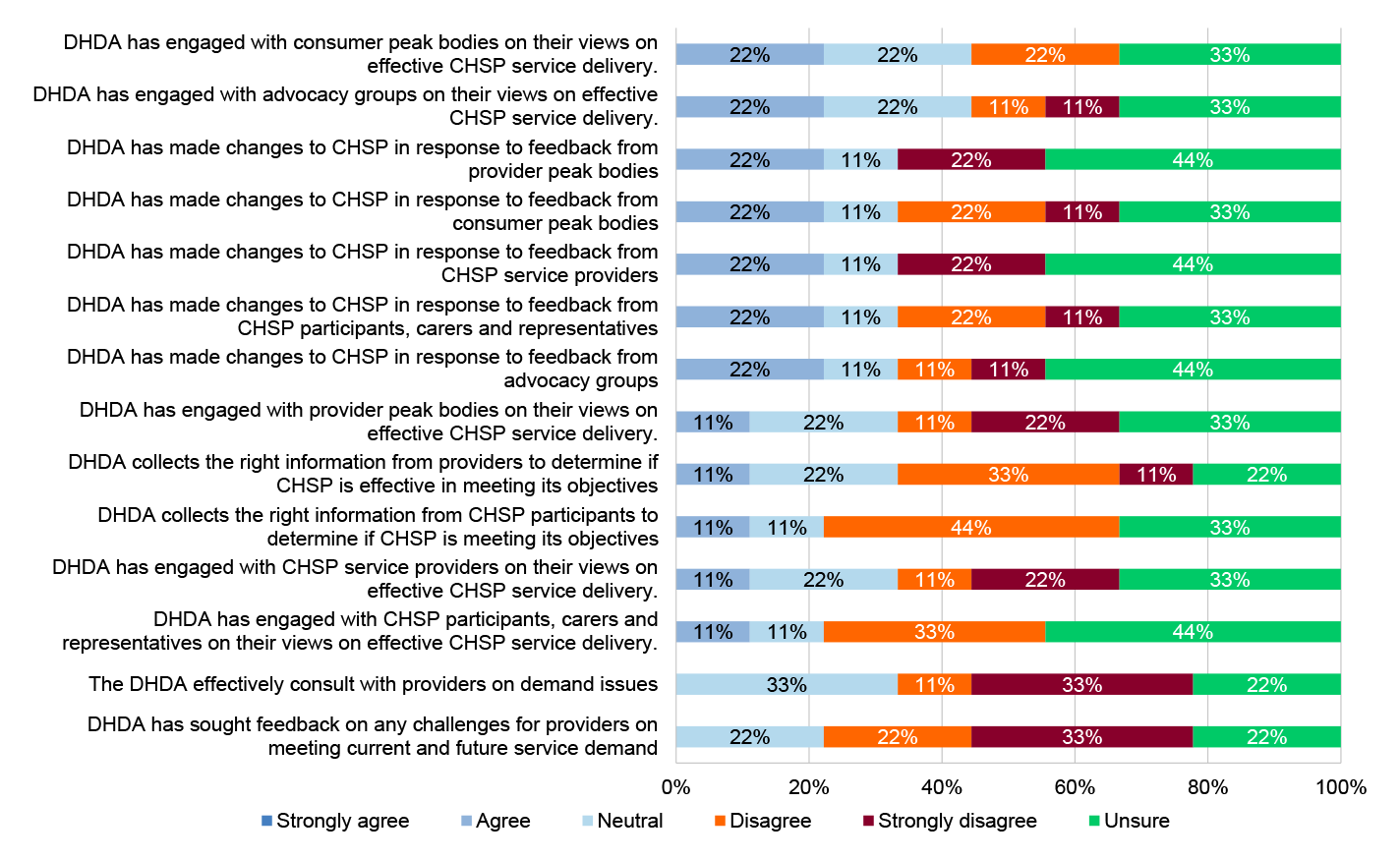
Source: ANAO peak body survey.
4. The survey included 10 free text questions. The key themes identified through the analysis of the free text responses are outlined in Table A.6.
Table A.6: Key themes from Commonwealth Home Support Program peak body survey responses
|
Key themes |
Key points identified |
|
Aged care reforms and CHSP transition |
Peak bodies noted that CHSP clients avoid transitioning to the Home Care Packages Program due to the higher client fees and remain in the CHSP with higher needs than the program is designed to meet and risk poorer outcomes. Peak bodies identified that the transition to Support at Home is creating uncertainties and anxiety for providers and participants. |
|
Assessment and eligibility |
Peak bodies reported they have received feedback that people experience difficulties with My Aged Care processes, including long wait times, difficulty finding providers with capacity and receiving incorrect information about their eligibility. Peak bodies raised concerns about inconsistencies with the single assessment process. |
|
Communication and engagement |
Peak bodies raised concerns that communication is inadequate and is not inclusive or accessible for older people. Peak bodies identified that terminology and advice can be inconsistent, causing further confusion with system changes. Peak bodies noted that there has been insufficient engagement with older people to understand the value of the CHSP and issues and gaps within the program. |
|
Cultural safety and diverse populations |
Peak bodies reported that they have received feedback that services may be culturally unsafe in some locations. Peak bodies noted that language barriers can reduce people’s access to, and uptake of, CHSP services. Peak bodies identified that funding constraints can make it very difficult to recruit and retain culturally safe staff. |
|
Demand and capacity |
Peak bodies raised concerns about services being at capacity and having long waiting lists. |
|
Funding |
Peak bodies identified concerns with funding being insufficient to meet client care and support needs, noting that this alongside funding uncertainty and short-term extensions has contributed to providers exiting the system. Peak bodies reported ‘postcode lotteries’ due to inconsistent national funding allocation that results in a person in one region being able to access multiple services and a person in another region is unable to access any support. Peak bodies reported positive aspects to the block funding model, noting challenges with lack of flexibility and when client demand is higher than anticipated or funded between grant rounds. |
|
Rural and remote |
Peak bodies noted that rural and remote providers can have additional challenges with reliably being able to staff their services, which can reduce service coverage and continuity for clients. |
|
Transparency and reporting |
Peak bodies identified concerns with the lack of national visibility on waiting lists and a lack of real-time, quality data on demand and service gaps. Peak bodies stated that provider reporting is focused on outputs they deliver and compliance-focused and does not identify unmet demand or client outcomes. This impacts program planning and commissioning services and can result in misallocation and slow responses to service gaps. Peak bodies also noted that providers can perceive reporting as burdensome, especially as it is insufficient to support planning or compare performance. |
|
Workforce |
Peak bodies raised concerns that providers are constrained by short-term funding arrangements resulting in difficulty in providing job security. This in turn impacts staff retention and the quality of service delivery. Peak bodies noted that they have received reports of volunteer shortages. |
Source: ANAO CHSP peak body survey.
5. In addition to the survey responses, the ANAO received 11 submissions from peak bodies through the public contribution function on the ANAO website (see paragraph 1.20) and met with three peak bodies.
Appendix 6 Commonwealth Home Support Program client survey
1. The Commonwealth Home Support Program (CHSP) client survey was conducted by the Social Research Centre on behalf of the ANAO.
2. The survey employed an online methodology, with survey invitations delivered by email. The ANAO acknowledges that an exclusively online survey conducted by email invitation does not reach clients who do not have access to an email account or the Internet. Further, it risks lower engagement in the survey among older CHSP clients and those with additional needs or support requirements. In addition, as noted below, the survey did not include CHSP clients who have not undergone an aged care assessment, as the Department of Health, Disability and Ageing (DHDA) does not hold contact details for unassessed clients. These methodological limitations create potential non-response bias in the final sample and results. To help mitigate this risk, carers or support contacts were invited to complete the survey on behalf of CHSP clients as a proxy respondent. The Social Research Centre provided a helpdesk and 1800 number throughout the fieldwork period. In total the helpdesk received 582 contacts by telephone and 1,124 contacts by email. Data weights by age group (and other demographic characteristics) were applied to help improve the representativeness of the sample.
3. The in-scope population for the client survey included anyone who had received a positive assessment outcome to enrol as a CHSP client and for whom DHDA had an email address on record. The population list was provided by DHDA to the ANAO and included N=317,645 records. After cleansing, which involved de-duplicating contact details, testing the validity of email addresses and removing records with insufficient contact details, the population list contained N=302,252 records.
4. The survey was voluntary and informed consent was obtained from all survey participants. Clients were assured in all survey correspondence and materials that they were not required to complete the survey and that their information would be treated confidentially.
5. Survey methodology employed unique links for each client to enable monitoring of survey participation and management of the reminder email schedule throughout fieldwork. A two-stage random sample was selected.122 Following discussions to identify groups of interest for the research, an initial sample of n=66,667 ‘main’ sample records and a ‘reserve’ sample of n=33,333 records were selected. Based on fieldwork monitoring projections and target completions, an additional ‘boost’ sample of n=59,997 records was selected. The total sample selection was therefore n=159,997.
6. The main sample was sent a pre-notification email from the Social Research Centre that provided key information about the survey, such as the purpose, length, fieldwork dates, and privacy information.123 All email communications included an option for clients to unsubscribe from survey-related communications.
7. A soft launch to ensure the field-readiness of the survey was conducted on 17 November 2025, involving delivery of n=1,000 survey invitations, which yielded n=15 completed questionnaires. Given the critically low response rate, an investigation was conducted during which a survey error that affected a small number of respondents (n=11) was identified and resolved. Given that initial participant engagement was lower than expected, the full survey launch was paused to consider survey modifications designed to boost response rate. The changes implemented included deployment of the additional boost sample and the introduction of a ‘core’ questionnaire. The core questionnaire allowed CHSP clients who were not currently receiving any services to respond to certain relevant questions.
8. The main fieldwork period was 20 November 2025 to 7 December 2025, with the sample being progressively initiated throughout fieldwork based on response performance and estimates. A total of n=159,997 survey invitations were delivered over the course of fieldwork. Three reminders were sent to the main sample, two reminders were sent to the reserve sample, and no reminders were sent to the boost sample.
9. The average time taken to complete the survey questionnaire was 10.9 minutes.
10. After quality assurance procedures, n=59 completed survey responses were excluded from the final data. A total of n=10,125 surveys were successfully completed, representing a response rate of 6.5 per cent. The overall number of completed questionnaires comprised n=9,025 responses to the full questionnaire and n=1,100 responses to the core questionnaire. In total, n=8,200 questionnaires were completed by CHSP clients, while n=1,925 questionnaires were completed by proxy respondents.
11. A weight was calculated for each respondent so that the distributions of respondents aligned with the population distributions on key characteristics, comprising: age group, Aboriginal or Torres Strait Islander status, country of birth, gender, state, capital city versus rest of state, and SEIFA IRSD124 quintile.
12. With weighting applied to a sample size of 10,125, the effective sample size is 8,393. Estimates of proportions at the overall level are generally accurate to within a margin of error of ±1.1 percentage points at a 95 per cent confidence level. All margin of error values for demographic estimates are within 1.1 per cent, with smaller values where estimates are closer to zero per cent or 100 per cent (e.g. see First nations status). It is expected that other estimates of proportions will yield similar margin of error values.
13. The client survey results are presented in Table A.7 to Table A.74. All reported percentages are based on weighted data. All reported counts (n=) are based on unweighted data.
Table A.7: Are you completing this survey as someone who receives aged care services in your home or community, or completing on behalf of someone who receives aged care services in their home or community?
|
Option |
n= |
Percentage (%) |
|
I receive aged care services in my home or community |
7,210 |
71.2 |
|
I am responding on behalf of someone who receives aged care services in their home or community |
1,813 |
17.9 |
|
Neithera |
1,100 |
10.9 |
|
Total |
10,125 |
100 |
Note a: This option captures CHSP clients who are not receiving any services through the CHSP due to availability issues in their area. Respondents not receiving any services through the CHSP answered a short ‘core’ questionnaire that excluded questions relating to quality of services and impact of the CHSP.
Source: CHSP client survey.
Table A.8: Before participating in this survey, had you heard of the Commonwealth Home Support Program?
|
Option |
n= |
Percentage (%) |
|
Yes |
8,871 |
87.7 |
|
No |
1,238 |
12.2 |
|
Not sure |
16 |
0.1 |
|
Prefer not to answer |
0 |
– |
|
Total |
10,125 |
100 |
Source: CHSP client survey.
Table A.9: Which of the following aged care services have you received in your home or community from a local provider in the last 6 monthsa
|
Option |
Number of respondents reporting each service |
Percentage of clients reporting each service |
|
Cleaning, laundry, and other household chores |
5,286 |
58.4 |
|
Home or garden maintenance |
2,796 |
31.3 |
|
Podiatry, physiotherapy, and other therapies |
2,480 |
27.6 |
|
Aids to stay independent |
1,681 |
18.1 |
|
Transport |
1,646 |
18.7 |
|
Changes to my home to improve accessibility |
1,488 |
16.3 |
|
Meals and food preparation |
1,400 |
15.8 |
|
Social outings |
878 |
10.3 |
|
Help with incontinence |
822 |
9.3 |
|
Bathing, hygiene, and grooming |
592 |
7.1 |
|
Nursing |
443 |
4.8 |
|
Help with impairments |
263 |
2.9 |
|
Day or overnight respite care |
217 |
2.6 |
|
I haven’t received any of these services in the last 6 months |
1,026 |
11.2 |
|
Not sure |
4 |
0.0 |
|
Prefer not to answer |
1 |
0.0 |
|
Total respondents |
9,025 |
N/A |
Note a: Asked of respondents receiving aged care services in their home or community or responding on behalf of someone who receives services.
Source: CHSP client survey.
Table A.10: How long have you been receiving aged care services in your home from a local provider?a
|
Option |
n= |
Percentage (%) |
|
Less than 3 months |
795 |
10.2 |
|
3 to less than 6 months |
1,008 |
12.9 |
|
6 to less than 12 months |
1,563 |
19.6 |
|
1 year to less than 2 years |
2,294 |
28.8 |
|
2 years or more |
2,305 |
28.0 |
|
Not sure |
13 |
0.2 |
|
Prefer not to answer |
16 |
0.2 |
|
Total |
7,994 |
100 |
Note a: Asked of respondents who had received aged care services in the last six months.
Source: CHSP client survey.
Table A.11: Do you recall applying for an assessment through My Aged Care?
|
Option |
n= |
Percentage (%) |
|
Yes |
9,819 |
97.0 |
|
No |
300 |
3.0 |
|
Not sure |
6 |
0.1 |
|
Prefer not to answer |
0 |
– |
|
Total |
10,125 |
100 |
Source: CHSP client survey.
Table A.12: Are you currently on a waitlist for a Home Care Package?
|
Option |
n= |
Percentage (%) |
|
Yes |
2,730 |
27.8 |
|
No |
7,315 |
71.5 |
|
Not sure |
74 |
0.7 |
|
Prefer not to answer |
6 |
0.1 |
|
Total |
10,125 |
100 |
Source: CHSP client survey.
Table A.13: How long did you have to wait between applying for an assessment for aged care services and getting an assessment outcome?a
|
Option |
n= |
Percentage (%) |
|
Less than 1 month |
1,573 |
15.6 |
|
1 to less than 3 months |
3,118 |
31.0 |
|
3 to less than 6 months |
1,885 |
19.3 |
|
6 to less than 12 months |
1,545 |
16.0 |
|
12 to less than 18 months |
846 |
9.1 |
|
18 months to less than 2 years |
365 |
4.0 |
|
2 years or more |
378 |
4.0 |
|
Not sure |
96 |
0.9 |
|
Prefer not to answer |
19 |
0.2 |
|
Total |
9,710 |
99 |
Note a: Asked of respondents who recall applying for an assessment through My Aged Care, are not sure or ‘prefer not to say’.
Source: CHSP client survey.
Table A.14: How long did you have to wait between being approved for aged care services and receiving the aged care services?a
|
Option |
n= |
Percentage (%) |
|
Less than 1 month |
1,548 |
17.1 |
|
1 to less than 3 months |
2,886 |
32.5 |
|
3 to less than 6 months |
1,596 |
18.2 |
|
6 to less than 12 months |
1,221 |
14.5 |
|
12 to less than 18 months |
614 |
7.5 |
|
18 months to less than 2 years |
270 |
3.1 |
|
2 years or more |
380 |
4.5 |
|
Not sure |
185 |
2.2 |
|
Prefer not to answer |
40 |
0.4 |
|
Total |
8,740 |
100 |
Note a: Asked of either those receiving aged care services themselves, or answering on behalf of someone who does and those who recall applying for an assessment through My Aged Care, or not sure or prefer not to say.
Source: CHSP client survey.
Table A.15: How much do you agree or disagree that the waiting times to receive aged care services in your home were reasonable?
|
Option |
n= |
Percentage (%) |
|
Strongly agree |
1,068 |
10.0 |
|
Agree |
2,625 |
25.6 |
|
Neither agree nor disagree |
2,214 |
22.2 |
|
Disagree |
1,917 |
19.1 |
|
Strongly disagree |
2,268 |
22.8 |
|
Not sure |
24 |
0.2 |
|
Prefer not to answer |
9 |
0.1 |
|
Total |
10,125 |
100 |
Source: CHSP client survey.
Table A.16: Thinking about your local area, in general how easy or difficult is it to receive aged care services in your home when you need them?
|
Option |
n= |
Percentage (%) |
|
Very easy |
944 |
9.2 |
|
Somewhat easy |
1,903 |
18.4 |
|
Neither easy nor difficult |
2,041 |
20.5 |
|
Somewhat difficult |
2,665 |
26.4 |
|
Very difficult |
2,453 |
24.5 |
|
Not sure |
104 |
0.9 |
|
Prefer not to answer |
15 |
0.2 |
|
Total |
10,125 |
100 |
Source: CHSP client survey.
Table A.17: Thinking about the first time you received a [each service] in your home or community from a local provider, how easy or difficult was it to get someone to provide that service?a
|
Service |
Average scoreb |
n= |
|
Meals and food preparation |
2.0 |
1,389 |
|
Bathing, hygiene, and grooming |
2.4 |
591 |
|
Nursing |
2.2 |
441 |
|
Podiatry, physiotherapy, and other therapies |
2.4 |
2,474 |
|
Help with impairments |
2.4 |
263 |
|
Help with incontinence |
2.4 |
818 |
|
Day or overnight respite care |
2.8 |
213 |
|
Changes to my home to improve accessibility |
2.6 |
1,487 |
|
Home or garden maintenance |
2.8 |
2,792 |
|
Cleaning, laundry, and other household chores |
2.6 |
5,278 |
|
Aids to stay independent |
2.5 |
1,675 |
|
Transport |
2.1 |
1,635 |
|
Social outings |
2.0 |
872 |
Note a: Asked of those who reported receiving the service.
Note b: 1 — very easy, 2 — somewhat easy, 3 — neither easy nor difficult, 4 — somewhat difficult, 5 — very difficult.
Source: CHSP client survey.
Table A.18: Thinking about the first time you received a meals and food preparation service in your home or community from a local provider, how easy or difficult was it to get someone to provide that service?a
|
Option |
n= |
Percentage (%) |
|
Very easy |
606 |
43.1 |
|
Somewhat easy |
467 |
32.5 |
|
Neither easy nor difficult |
157 |
12.3 |
|
Somewhat difficult |
113 |
8.3 |
|
Very difficult |
46 |
3.0 |
|
Not sure |
5 |
0.5 |
|
Prefer not to answer |
6 |
0.4 |
|
Total |
1,400 |
100 |
Note a: Asked of those who reported receiving the service.
Source: CHSP client survey.
Table A.19: Thinking about the first time you received a bathing, hygiene and grooming service in your home or community from a local provider, how easy or difficult was it to get someone to provide that service?a
|
Option |
n= |
Percentage (%) |
|
Very easy |
163 |
26.9 |
|
Somewhat easy |
219 |
35.8 |
|
Neither easy nor difficult |
82 |
14.5 |
|
Somewhat difficult |
90 |
17.1 |
|
Very difficult |
37 |
5.6 |
|
Not sure |
1 |
0.1 |
|
Prefer not to answer |
0 |
– |
|
Total |
592 |
100 |
Note a: Asked of those who reported receiving the service.
Source: CHSP client survey.
Table A.20: Thinking about the first time you received a nursing service in your home or community from a local provider, how easy or difficult was it to get someone to provide that service?a
|
Option |
n= |
Percentage (%) |
|
Very easy |
166 |
36.2 |
|
Somewhat easy |
139 |
30.7 |
|
Neither easy nor difficult |
60 |
14.9 |
|
Somewhat difficult |
58 |
13.2 |
|
Very difficult |
18 |
4.5 |
|
Not sure |
1 |
0.2 |
|
Prefer not to answer |
1 |
0.2 |
|
Total |
443 |
100 |
Note a: Asked of those who reported receiving the service.
Source: CHSP client survey.
Table A.21: Thinking about the first time you received a podiatry, physiotherapy, and other therapies service in your home or community from a local provider, how easy or difficult was it to get someone to provide that service?a
|
Option |
n= |
Percentage (%) |
|
Very easy |
744 |
29.7 |
|
Somewhat easy |
833 |
33.3 |
|
Neither easy nor difficult |
356 |
15.0 |
|
Somewhat difficult |
382 |
15.3 |
|
Very difficult |
159 |
6.6 |
|
Not sure |
4 |
0.1 |
|
Prefer not to answer |
2 |
0.1 |
|
Total |
2,480 |
100 |
Note a: Asked of those who reported receiving the service.
Source: CHSP client survey.
Table A.22: Thinking about the first time you received a help with impairments service in your home or community from a local provider, how easy or difficult was it to get someone to provide that service?a
|
Option |
n= |
Percentage (%) |
|
Very easy |
52 |
21.5 |
|
Somewhat easy |
96 |
35.8 |
|
Neither easy nor difficult |
62 |
24.4 |
|
Somewhat difficult |
39 |
13.8 |
|
Very difficult |
14 |
4.5 |
|
Not sure |
0 |
– |
|
Prefer not to answer |
0 |
– |
|
Total |
263 |
100 |
Note a: Asked of those who reported receiving the service.
Source: CHSP client survey.
Table A.23: Thinking about the first time you received a help with incontinence service in your home or community from a local provider, how easy or difficult was it to get someone to provide that service?a
|
Option |
n= |
Percentage (%) |
|
Very easy |
227 |
26.9 |
|
Somewhat easy |
274 |
33.8 |
|
Neither easy nor difficult |
153 |
18.9 |
|
Somewhat difficult |
120 |
14.6 |
|
Very difficult |
44 |
5.4 |
|
Not sure |
3 |
0.3 |
|
Prefer not to answer |
1 |
0.2 |
|
Total |
822 |
100 |
Note a: Asked of those who reported receiving the service.
Source: CHSP client survey.
Table A.24: Thinking about the first time you received a day or overnight respite service in your home or community from a local provider, how easy or difficult was it to get someone to provide that service?a
|
Option |
n= |
Percentage (%) |
|
Very easy |
34 |
14.3 |
|
Somewhat easy |
69 |
33.3 |
|
Neither easy nor difficult |
46 |
19.1 |
|
Somewhat difficult |
40 |
17.8 |
|
Very difficult |
24 |
13.0 |
|
Not sure |
3 |
2.2 |
|
Prefer not to answer |
1 |
0.4 |
|
Total |
217 |
100 |
Note a: Asked of those who reported receiving the service.
Source: CHSP client survey.
Table A.25: Thinking about the first time you received a changes to my home to improve accessibility service in your home or community from a local provider, how easy or difficult was it to get someone to provide that service?a
|
Option |
n= |
Percentage (%) |
|
Very easy |
325 |
21.5 |
|
Somewhat easy |
492 |
32.9 |
|
Neither easy nor difficult |
258 |
17.9 |
|
Somewhat difficult |
284 |
19.2 |
|
Very difficult |
128 |
8.5 |
|
Not sure |
0 |
– |
|
Prefer not to answer |
1 |
0.0 |
|
Total |
1,488 |
100 |
Note a: Asked of those who reported receiving the service.
Source: CHSP client survey.
Table A.26: Thinking about the first time you received a home or garden maintenance service in your home or community from a local provider, how easy or difficult was it to get someone to provide that service?a
|
Option |
n= |
Percentage (%) |
|
Very easy |
636 |
22.2 |
|
Somewhat easy |
798 |
28.7 |
|
Neither easy nor difficult |
382 |
14.2 |
|
Somewhat difficult |
586 |
20.2 |
|
Very difficult |
390 |
14.6 |
|
Not sure |
3 |
0.1 |
|
Prefer not to answer |
1 |
0.0 |
|
Total |
2,796 |
100 |
Note a: Asked of those who reported receiving the service.
Source: CHSP client survey.
Table A.27: Thinking about the first time you received a cleaning, laundry and other household chores service in your home or community from a local provider, how easy or difficult was it to get someone to provide that service?a
|
Option |
n= |
Percentage (%) |
|
Very easy |
1,281 |
23.8 |
|
Somewhat easy |
1,707 |
31.5 |
|
Neither easy nor difficult |
917 |
17.6 |
|
Somewhat difficult |
953 |
18.5 |
|
Very difficult |
420 |
8.5 |
|
Not sure |
4 |
0.1 |
|
Prefer not to answer |
4 |
0.1 |
|
Total |
5,286 |
100 |
Note a: Asked of those who reported receiving the service.
Source: CHSP client survey.
Table A.28: Thinking about the first time you received an aids to stay independent service in your home or community from a local provider, how easy or difficult was it to get someone to provide that service?a
|
Option |
n= |
Percentage (%) |
|
Very easy |
421 |
24.9 |
|
Somewhat easy |
567 |
32.8 |
|
Neither easy nor difficult |
312 |
19.8 |
|
Somewhat difficult |
255 |
15.0 |
|
Very difficult |
120 |
7.1 |
|
Not sure |
2 |
0.1 |
|
Prefer not to answer |
4 |
0.2 |
|
Total |
1,681 |
100 |
Note a: Asked of those who reported receiving the service.
Source: CHSP client survey.
Table A.29: Thinking about the first time you received a transport service in your home or community from a local provider, how easy or difficult was it to get someone to provide that service?a
|
Option |
n= |
Percentage (%) |
|
Very easy |
623 |
36.8 |
|
Somewhat easy |
522 |
33.0 |
|
Neither easy nor difficult |
219 |
13.1 |
|
Somewhat difficult |
191 |
11.8 |
|
Very difficult |
80 |
4.6 |
|
Not sure |
8 |
0.6 |
|
Prefer not to answer |
3 |
0.2 |
|
Total |
1,646 |
100 |
Note a: Asked of those who reported receiving the service.
Source: CHSP client survey.
Table A.30: Thinking about the first time you received a social outings service in your home or community from a local provider, how easy or difficult was it to get someone to provide that service?a
|
Option |
n= |
Percentage (%) |
|
Very easy |
342 |
38.4 |
|
Somewhat easy |
303 |
34.7 |
|
Neither easy nor difficult |
118 |
13.9 |
|
Somewhat difficult |
80 |
9.1 |
|
Very difficult |
29 |
3.3 |
|
Not sure |
5 |
0.6 |
|
Prefer not to answer |
1 |
0.1 |
|
Total |
878 |
100 |
Note a: Asked of those who reported receiving the service.
Source: CHSP client survey.
Table A.31: Average scoresa for client satisfaction with services against the following aspectsb
|
|
Overall quality of the service provided |
Alignment of the service to your care plan |
Service met your needs |
Staff arrived when they said they would |
Professionalism of service staff |
How the staff communicated with you |
Staff respected your cultural or personal identity |
Kindness and compassion shown by staff |
Service was completed |
|||||||||
|
|
Score |
n= |
Score |
n= |
Score |
n= |
Score |
n= |
Score |
n= |
Score |
n= |
Score |
n= |
Score |
n= |
Score |
n= |
|
Meals and food preparation |
2.0 |
1,386 |
2.0 |
1,382 |
2.0 |
1,389 |
1.8 |
1,367 |
1.7 |
1,373 |
2.0 |
1,386 |
2.0 |
1,382 |
2.0 |
1,389 |
1.8 |
1,367 |
|
Bathing, hygiene, and grooming |
1.7 |
592 |
1.9 |
592 |
1.8 |
592 |
1.7 |
592 |
1.6 |
592 |
1.7 |
592 |
1.9 |
592 |
1.8 |
592 |
1.7 |
592 |
|
Nursing |
1.7 |
442 |
1.9 |
442 |
1.8 |
442 |
1.7 |
440 |
1.6 |
440 |
1.7 |
442 |
1.9 |
442 |
1.8 |
442 |
1.7 |
440 |
|
Podiatry, physiotherapy, and other therapies |
1.7 |
2,472 |
1.9 |
2,458 |
1.8 |
2,468 |
1.7 |
2,455 |
1.5 |
2,468 |
1.7 |
2,472 |
1.9 |
2,458 |
1.8 |
2,468 |
1.7 |
2,455 |
|
Help with impairments |
1.9 |
263 |
2.0 |
263 |
2.0 |
263 |
1.7 |
262 |
1.7 |
262 |
1.9 |
263 |
2.0 |
263 |
2.0 |
263 |
1.7 |
262 |
|
Help with incontinence |
1.9 |
818 |
2.0 |
809 |
2.0 |
819 |
1.9 |
804 |
1.8 |
807 |
1.9 |
818 |
2.0 |
809 |
2.0 |
819 |
1.9 |
804 |
|
Day or overnight respite care |
1.9 |
214 |
2.0 |
214 |
2.0 |
214 |
1.8 |
212 |
1.7 |
212 |
1.9 |
214 |
2.0 |
214 |
2.0 |
214 |
1.8 |
212 |
|
Changes to my home to improve accessibility |
1.8 |
1,482 |
1.9 |
1,478 |
1.9 |
1,482 |
1.7 |
1,485 |
1.7 |
1,484 |
1.8 |
1,482 |
1.9 |
1,478 |
1.9 |
1,482 |
1.7 |
1,485 |
|
Home or garden maintenance |
2.0 |
2,786 |
2.1 |
2,775 |
2.0 |
2,788 |
1.8 |
2,784 |
1.8 |
2,785 |
2.0 |
2,786 |
2.1 |
2,775 |
2.0 |
2,788 |
1.8 |
2,784 |
|
Cleaning, laundry, and other household chores |
1.9 |
5,276 |
2.0 |
5,256 |
2.0 |
5,277 |
1.8 |
5,278 |
1.7 |
5,278 |
1.9 |
5,276 |
2.0 |
5,256 |
2.0 |
5,277 |
1.8 |
5,278 |
|
Aids to stay independent |
1.9 |
1,671 |
2.0 |
1,671 |
2.0 |
1,672 |
1.8 |
1,669 |
1.7 |
1,671 |
1.9 |
1,671 |
2.0 |
1,671 |
2.0 |
1,672 |
1.8 |
1,669 |
|
Transport |
1.7 |
1,636 |
1.8 |
1,631 |
1.8 |
1,636 |
1.7 |
1,634 |
1.6 |
1,634 |
1.7 |
1,636 |
1.8 |
1,631 |
1.8 |
1,636 |
1.7 |
1,634 |
|
Social outings |
1.7 |
875 |
1.8 |
872 |
1.7 |
874 |
1.7 |
870 |
1.5 |
871 |
1.7 |
875 |
1.8 |
872 |
1.7 |
874 |
1.7 |
870 |
Note a: 1 — very satisfied, 2 — satisfied, 3 — neither satisfied nor dissatisfied, 4 — dissatisfied, 5 — very dissatisfied.
Note b: Asked of those who reported receiving the service.
Source: CHSP client survey.
Table A.32: Thinking about the most recent time you received a meals and food preparation service in your home or community from a local provider, how satisfied or dissatisfied were you with the following aspects?a
|
|
|
Very satisfied |
Satisfied |
Neither satisfied nor dissatisfied |
Dissatisfied |
Very dissatisfied |
Not sure |
Prefer not to answer |
|
The overall quality of the service provided |
% |
33.3 |
43.7 |
12.2 |
6.3 |
3.3 |
0.9 |
0.4 |
|
n= |
487 |
601 |
162 |
91 |
45 |
9 |
5 |
|
|
Alignment of the service to your care plan |
% |
32.5 |
44.4 |
14.1 |
4.3 |
3.1 |
1.2 |
0.4 |
|
n= |
466 |
630 |
184 |
62 |
40 |
13 |
5 |
|
|
The service provided met your needs |
% |
34.1 |
41.4 |
12.5 |
7.6 |
3.4 |
0.6 |
0.3 |
|
n= |
483 |
590 |
162 |
108 |
46 |
7 |
4 |
|
|
Staff arrived when they said they would |
% |
44.8 |
36.0 |
12.9 |
2.3 |
1.8 |
1.5 |
0.9 |
|
n= |
621 |
506 |
188 |
32 |
20 |
18 |
15 |
|
|
The professionalism of the service staff |
% |
46.5 |
36.5 |
12.1 |
1.3 |
1.7 |
1.3 |
0.6 |
|
n= |
657 |
516 |
163 |
20 |
17 |
16 |
11 |
|
|
How the staff communicated with you |
% |
47.6 |
35.7 |
11.2 |
1.7 |
1.8 |
1.3 |
0.8 |
|
n= |
666 |
513 |
148 |
24 |
21 |
16 |
12 |
|
|
The staff respected your cultural or personal identity |
% |
42.3 |
32.4 |
20.1 |
0.9 |
2.0 |
1.4 |
0.8 |
|
n= |
597 |
462 |
279 |
12 |
19 |
18 |
13 |
|
|
The kindness and compassion shown by staff |
% |
49.2 |
32.2 |
13.7 |
1.4 |
1.4 |
1.5 |
0.8 |
|
n= |
688 |
459 |
191 |
15 |
16 |
19 |
12 |
|
|
The service they were meant to provide was completed |
% |
38.5 |
45.3 |
9.6 |
3.1 |
2.5 |
0.7 |
0.4 |
|
n= |
546 |
632 |
134 |
44 |
31 |
8 |
5 |
|
Note a: Asked of those who reported receiving the service.
Source: CHSP client survey.
Table A.33: Thinking about the most recent time you received a bathing and hygiene service in your home or community from a local provider, how satisfied or dissatisfied were you with the following aspects?a
|
|
|
Very satisfied |
Satisfied |
Neither satisfied nor dissatisfied |
Dissatisfied |
Very dissatisfied |
Not sure |
Prefer not to answer |
|
The overall quality of the service provided |
% |
46.1 |
40.6 |
7.4 |
4.0 |
1.8 |
– |
– |
|
n= |
280 |
233 |
45 |
24 |
10 |
0 |
0 |
|
|
Alignment of the service to your care plan |
% |
37.3 |
45.2 |
11.1 |
4.3 |
2.1 |
– |
– |
|
n= |
227 |
261 |
67 |
25 |
12 |
0 |
0 |
|
|
The service provided met your needs |
% |
43.8 |
41.3 |
7.8 |
4.8 |
2.3 |
– |
– |
|
n= |
263 |
239 |
50 |
26 |
14 |
0 |
0 |
|
|
Staff arrived when they said they would |
% |
47.7 |
39.2 |
7.5 |
3.7 |
2.0 |
– |
– |
|
n= |
286 |
226 |
45 |
24 |
11 |
0 |
0 |
|
|
The professionalism of the service staff |
% |
58.0 |
33.0 |
6.2 |
1.4 |
1.4 |
– |
– |
|
n= |
348 |
190 |
38 |
8 |
8 |
0 |
0 |
|
|
How the staff communicated with you |
% |
56.3 |
33.3 |
6.0 |
2.5 |
2.0 |
– |
– |
|
n= |
336 |
194 |
34 |
17 |
11 |
0 |
0 |
|
|
The staff respected your cultural or personal identity |
% |
57.0 |
32.1 |
8.7 |
0.8 |
1.2 |
– |
0.1 |
|
n= |
342 |
187 |
51 |
5 |
6 |
0 |
1 |
|
|
The kindness and compassion shown by staff |
% |
62.8 |
29.5 |
4.9 |
1.5 |
1.3 |
– |
– |
|
n= |
376 |
172 |
27 |
9 |
8 |
0 |
0 |
|
|
The service they were meant to provide was completed |
% |
43.5 |
44.1 |
7.0 |
3.7 |
1.8 |
– |
– |
|
n= |
264 |
252 |
44 |
22 |
10 |
0 |
0 |
|
Note a: Asked of those who reported receiving the service.
Source: CHSP client survey.
Table A.34: Thinking about the most recent time you received a nursing service in your home or community from a local provider, how satisfied or dissatisfied were you with the following aspects?a
|
|
|
Very satisfied |
Satisfied |
Neither satisfied nor dissatisfied |
Dissatisfied |
Very dissatisfied |
Not sure |
Prefer not to answer |
|
The overall quality of the service provided |
% |
50.1 |
35.9 |
7.2 |
4.1 |
2.6 |
0.2 |
– |
|
n= |
233 |
151 |
31 |
15 |
12 |
1 |
0 |
|
|
Alignment of the service to your care plan |
% |
41.8 |
36.0 |
14.7 |
4.1 |
3.2 |
0.2 |
– |
|
n= |
198 |
151 |
62 |
16 |
15 |
1 |
0 |
|
|
The service provided met your needs |
% |
47.9 |
34.9 |
8.8 |
4.4 |
3.7 |
0.2 |
– |
|
n= |
225 |
145 |
40 |
16 |
16 |
1 |
0 |
|
|
Staff arrived when they said they would |
% |
47.3 |
37.8 |
10.3 |
1.8 |
2.0 |
0.6 |
0.3 |
|
n= |
223 |
155 |
45 |
7 |
10 |
2 |
1 |
|
|
The professionalism of the service staff |
% |
59.2 |
30.7 |
5.0 |
2.6 |
1.7 |
0.6 |
0.3 |
|
n= |
268 |
132 |
24 |
9 |
7 |
2 |
1 |
|
|
How the staff communicated with you |
% |
56.5 |
31.7 |
7.7 |
1.1 |
2.2 |
0.6 |
0.3 |
|
n= |
256 |
137 |
32 |
6 |
9 |
2 |
1 |
|
|
The staff respected your cultural or personal identity |
% |
55.0 |
31.7 |
8.8 |
1.3 |
1.6 |
1.0 |
0.5 |
|
n= |
254 |
133 |
38 |
5 |
7 |
4 |
2 |
|
|
The kindness and compassion shown by staff |
% |
59.1 |
32.5 |
4.8 |
1.7 |
1.0 |
0.6 |
0.3 |
|
n= |
273 |
134 |
21 |
7 |
5 |
2 |
1 |
|
|
The service they were meant to provide was completed |
% |
47.2 |
37.9 |
6.2 |
4.7 |
3.5 |
0.4 |
0.1 |
|
n= |
219 |
158 |
28 |
19 |
16 |
2 |
1 |
|
Note a: Asked of those who reported receiving the service.
Source: CHSP client survey.
Table A.35: Thinking about the most recent time you received a podiatry, physiotherapy and other therapies service in your home or community from a local provider, how satisfied or dissatisfied were you with the following aspects?a
|
|
|
Very satisfied |
Satisfied |
Neither satisfied nor dissatisfied |
Dissatisfied |
Very dissatisfied |
Not sure |
Prefer not to answer |
|
The overall quality of the service provided |
% |
49.2 |
37.8 |
8.1 |
2.1 |
2.5 |
0.1 |
0.1 |
|
n= |
1,246 |
925 |
190 |
51 |
60 |
5 |
3 |
|
|
Alignment of the service to your care plan |
% |
39.2 |
41.3 |
13.4 |
2.9 |
2.4 |
0.6 |
0.2 |
|
n= |
992 |
1,021 |
316 |
66 |
63 |
17 |
5 |
|
|
The service provided met your needs |
% |
44.7 |
39.7 |
9.1 |
3.4 |
2.8 |
0.3 |
0.1 |
|
n= |
1,130 |
971 |
214 |
85 |
68 |
9 |
3 |
|
|
Staff arrived when they said they would |
% |
51.8 |
33.7 |
10.3 |
2.1 |
1.2 |
0.5 |
0.5 |
|
n= |
1,305 |
824 |
249 |
46 |
31 |
12 |
13 |
|
|
The professionalism of the service staff |
% |
59.1 |
33.0 |
5.1 |
1.1 |
1.3 |
0.2 |
0.2 |
|
n= |
1,485 |
802 |
120 |
26 |
35 |
7 |
5 |
|
|
How the staff communicated with you |
% |
56.2 |
34.8 |
5.7 |
1.6 |
1.1 |
0.3 |
0.3 |
|
n= |
1,417 |
841 |
144 |
35 |
29 |
7 |
7 |
|
|
The staff respected your cultural or personal identity |
% |
54.4 |
33.5 |
10.0 |
0.5 |
1.0 |
0.3 |
0.4 |
|
n= |
1,372 |
811 |
243 |
9 |
26 |
10 |
9 |
|
|
The kindness and compassion shown by staff |
% |
59.2 |
32.6 |
5.8 |
0.6 |
1.4 |
0.2 |
0.2 |
|
n= |
1,487 |
795 |
137 |
14 |
34 |
7 |
6 |
|
|
The service they were meant to provide was completed |
% |
44.1 |
39.5 |
10.3 |
2.9 |
2.8 |
0.4 |
0.2 |
|
n= |
1,116 |
969 |
242 |
66 |
70 |
12 |
5 |
|
Note a: Asked of those who reported receiving the service.
Source: CHSP client survey.
Table A.36: Thinking about the most recent time you received a help with impairments service in your home or community from a local provider, how satisfied or dissatisfied were you with the following aspects?a
|
|
|
Very satisfied |
Satisfied |
Neither satisfied nor dissatisfied |
Dissatisfied |
Very dissatisfied |
Not sure |
Prefer not to answer |
|
The overall quality of the service provided |
% |
37.6 |
43.4 |
13.2 |
3.2 |
2.6 |
– |
– |
|
n= |
97 |
113 |
34 |
10 |
9 |
0 |
0 |
|
|
Alignment of the service to your care plan |
% |
33.3 |
42.5 |
18.0 |
2.7 |
3.5 |
– |
– |
|
n= |
85 |
108 |
50 |
8 |
12 |
0 |
0 |
|
|
The service provided met your needs |
% |
35.0 |
43.9 |
14.1 |
3.1 |
3.9 |
– |
– |
|
n= |
88 |
114 |
37 |
10 |
14 |
0 |
0 |
|
|
Staff arrived when they said they would |
% |
48.1 |
38.5 |
9.5 |
2.5 |
0.8 |
0.6 |
– |
|
n= |
124 |
102 |
26 |
7 |
3 |
1 |
0 |
|
|
The professionalism of the service staff |
% |
48.1 |
38.8 |
10.1 |
1.8 |
0.7 |
0.6 |
– |
|
n= |
126 |
101 |
27 |
6 |
2 |
1 |
0 |
|
|
How the staff communicated with you |
% |
47.7 |
39.7 |
8.7 |
2.4 |
1.0 |
0.6 |
– |
|
n= |
121 |
107 |
23 |
8 |
3 |
1 |
0 |
|
|
The staff respected your cultural or personal identity |
% |
49.3 |
37.4 |
11.0 |
0.5 |
0.9 |
0.6 |
0.3 |
|
n= |
127 |
101 |
28 |
2 |
3 |
1 |
1 |
|
|
The kindness and compassion shown by staff |
% |
51.9 |
36.7 |
9.5 |
0.8 |
0.7 |
0.6 |
– |
|
n= |
135 |
97 |
25 |
3 |
2 |
1 |
0 |
|
|
The service they were meant to provide was completed |
% |
36.4 |
42.0 |
15.0 |
3.5 |
3.1 |
– |
– |
|
n= |
93 |
109 |
40 |
11 |
10 |
0 |
0 |
|
Note a: Asked of those who reported receiving the service.
Source: CHSP client survey.
Table A.37: Thinking about the most recent time you received a help with incontinence service in your home or community from a local provider, how satisfied or dissatisfied were you with the following aspects?a
|
|
|
Very satisfied |
Satisfied |
Neither satisfied nor dissatisfied |
Dissatisfied |
Very dissatisfied |
Not sure |
Prefer not to answer |
|
The overall quality of the service provided |
% |
37.4 |
41.1 |
13.8 |
4.3 |
3.0 |
0.2 |
0.3 |
|
n= |
310 |
338 |
113 |
34 |
23 |
2 |
2 |
|
|
Alignment of the service to your care plan |
% |
32.9 |
42.8 |
16.1 |
3.4 |
3.3 |
1.0 |
0.5 |
|
n= |
276 |
346 |
129 |
30 |
28 |
9 |
4 |
|
|
The service provided met your needs |
% |
35.5 |
42.7 |
13.6 |
4.2 |
3.7 |
0.1 |
0.3 |
|
n= |
302 |
343 |
107 |
38 |
29 |
1 |
2 |
|
|
Staff arrived when they said they would |
% |
39.3 |
34.6 |
20.0 |
2.5 |
1.7 |
0.8 |
1.1 |
|
n= |
331 |
275 |
161 |
22 |
15 |
7 |
11 |
|
|
The professionalism of the service staff |
% |
44.0 |
35.9 |
14.2 |
1.9 |
2.4 |
0.7 |
0.9 |
|
n= |
370 |
286 |
116 |
17 |
18 |
6 |
9 |
|
|
How the staff communicated with you |
% |
42.0 |
36.0 |
16.1 |
2.6 |
1.8 |
0.6 |
0.9 |
|
n= |
353 |
290 |
127 |
23 |
15 |
5 |
9 |
|
|
The staff respected your cultural or personal identity |
% |
42.1 |
35.9 |
17.3 |
1.5 |
1.1 |
1.1 |
1.0 |
|
n= |
352 |
293 |
135 |
14 |
9 |
9 |
10 |
|
|
The kindness and compassion shown by staff |
% |
46.6 |
34.1 |
14.3 |
1.8 |
1.4 |
0.9 |
0.9 |
|
n= |
386 |
281 |
112 |
16 |
11 |
7 |
9 |
|
|
The service they were meant to provide was completed |
% |
36.6 |
41.6 |
14.8 |
3.4 |
2.8 |
0.4 |
0.4 |
|
n= |
306 |
338 |
118 |
30 |
23 |
4 |
3 |
|
Note a: Asked of those who reported receiving the service.
Source: CHSP client survey.
Table A.38: Thinking about the most recent time you received a day or overnight respite care service in your home or community from a local provider, how satisfied or dissatisfied were you with the following aspects?a
|
|
|
Very satisfied |
Satisfied |
Neither satisfied nor dissatisfied |
Dissatisfied |
Very dissatisfied |
Not sure |
Prefer not to answer |
|
The overall quality of the service provided |
% |
39.9 |
38.9 |
13.0 |
2.7 |
3.2 |
2.3 |
– |
|
n= |
89 |
85 |
31 |
6 |
3 |
3 |
0 |
|
|
Alignment of the service to your care plan |
% |
31.6 |
42.2 |
15.8 |
5.6 |
2.6 |
2.3 |
– |
|
n= |
71 |
94 |
35 |
12 |
2 |
3 |
0 |
|
|
The service provided met your needs |
% |
34.7 |
40.4 |
13.2 |
5.9 |
3.5 |
2.3 |
– |
|
n= |
79 |
86 |
32 |
13 |
4 |
3 |
0 |
|
|
Staff arrived when they said they would |
% |
40.8 |
38.5 |
12.6 |
2.2 |
3.0 |
2.3 |
0.8 |
|
n= |
91 |
84 |
29 |
5 |
3 |
3 |
2 |
|
|
The professionalism of the service staff |
% |
47.4 |
36.5 |
8.9 |
1.7 |
2.5 |
2.3 |
0.8 |
|
n= |
104 |
81 |
21 |
4 |
2 |
3 |
2 |
|
|
How the staff communicated with you |
% |
46.7 |
34.5 |
10.9 |
2.4 |
2.5 |
2.3 |
0.8 |
|
n= |
105 |
73 |
25 |
7 |
2 |
3 |
2 |
|
|
The staff respected your cultural or personal identity |
% |
48.9 |
33.4 |
12.7 |
0.0 |
1.9 |
2.3 |
0.8 |
|
n= |
109 |
74 |
28 |
0 |
1 |
3 |
2 |
|
|
The kindness and compassion shown by staff |
% |
53.3 |
32.4 |
9.0 |
0.3 |
1.9 |
2.3 |
0.8 |
|
n= |
118 |
72 |
20 |
1 |
1 |
3 |
2 |
|
|
The service they were meant to provide was completed |
% |
34.0 |
42.5 |
13.0 |
4.3 |
4.0 |
2.3 |
– |
|
n= |
79 |
93 |
28 |
9 |
5 |
3 |
0 |
|
Note a: Asked of those who reported receiving the service.
Source: CHSP client survey.
Table A.39: Thinking about the most recent time you received a changes to home to improve accessibility service in your home or community from a local provider, how satisfied or dissatisfied were you with the following aspects?a
|
|
|
Very satisfied |
Satisfied |
Neither satisfied nor dissatisfied |
Dissatisfied |
Very dissatisfied |
Not sure |
Prefer not to answer |
|
The overall quality of the service provided |
% |
42.4 |
40.1 |
10.0 |
3.9 |
3.2 |
0.2 |
0.1 |
|
n= |
641 |
589 |
143 |
64 |
45 |
4 |
2 |
|
|
Alignment of the service to your care plan |
% |
36.3 |
42.2 |
14.0 |
4.1 |
2.8 |
0.4 |
0.2 |
|
n= |
561 |
601 |
207 |
66 |
43 |
7 |
3 |
|
|
The service provided met your needs |
% |
40.4 |
41.2 |
10.6 |
4.5 |
3.0 |
0.2 |
0.1 |
|
n= |
616 |
592 |
155 |
75 |
44 |
4 |
2 |
|
|
Staff arrived when they said they would |
% |
48.4 |
37.2 |
9.2 |
3.4 |
1.7 |
0.1 |
0.1 |
|
n= |
708 |
567 |
140 |
46 |
24 |
2 |
1 |
|
|
The professionalism of the service staff |
% |
49.6 |
36.5 |
9.2 |
3.0 |
1.5 |
0.1 |
0.1 |
|
n= |
735 |
546 |
135 |
45 |
23 |
2 |
2 |
|
|
How the staff communicated with you |
% |
47.9 |
37.4 |
9.8 |
2.6 |
2.0 |
0.1 |
0.1 |
|
n= |
705 |
561 |
144 |
42 |
32 |
2 |
2 |
|
|
The staff respected your cultural or personal identity |
% |
47.1 |
36.0 |
13.9 |
1.2 |
1.2 |
0.3 |
0.4 |
|
n= |
697 |
534 |
206 |
22 |
18 |
5 |
6 |
|
|
The kindness and compassion shown by staff |
% |
50.6 |
35.6 |
10.4 |
1.9 |
1.2 |
0.1 |
0.1 |
|
n= |
750 |
526 |
157 |
33 |
18 |
2 |
2 |
|
|
The service they were meant to provide was completed |
% |
42.0 |
38.2 |
9.5 |
6.2 |
3.7 |
0.2 |
0.1 |
|
n= |
635 |
555 |
137 |
97 |
58 |
4 |
2 |
|
Note a: Asked of those who reported receiving the service.
Source: CHSP client survey.
Table A.40: Thinking about the most recent time you received a home or garden maintenance service in your home or community from a local provider, how satisfied or dissatisfied were you with the following aspects?a
|
|
|
Very satisfied |
Satisfied |
Neither satisfied nor dissatisfied |
Dissatisfied |
Very dissatisfied |
Not sure |
Prefer not to answer |
|
The overall quality of the service provided |
% |
40.6 |
37.4 |
10.8 |
6.1 |
4.7 |
0.2 |
0.2 |
|
n= |
1,155 |
1,031 |
296 |
180 |
124 |
5 |
5 |
|
|
Alignment of the service to your care plan |
% |
35.5 |
38.4 |
14.7 |
5.8 |
4.9 |
0.6 |
0.2 |
|
n= |
1,006 |
1,074 |
405 |
161 |
129 |
14 |
7 |
|
|
The service provided met your needs |
% |
38.3 |
37.4 |
10.8 |
7.8 |
5.3 |
0.2 |
0.1 |
|
n= |
1,089 |
1,031 |
298 |
229 |
141 |
4 |
4 |
|
|
Staff arrived when they said they would |
% |
46.4 |
35.1 |
9.7 |
4.7 |
3.6 |
0.3 |
0.2 |
|
n= |
1,329 |
969 |
261 |
123 |
102 |
6 |
6 |
|
|
The professionalism of the service staff |
% |
47.5 |
34.4 |
11.2 |
3.4 |
3.1 |
0.3 |
0.2 |
|
n= |
1,358 |
945 |
299 |
101 |
82 |
6 |
5 |
|
|
How the staff communicated with you |
% |
48.2 |
35.4 |
9.7 |
3.4 |
2.9 |
0.3 |
0.2 |
|
n= |
1,372 |
970 |
267 |
93 |
83 |
6 |
5 |
|
|
The staff respected your cultural or personal identity |
% |
48.1 |
34.0 |
14.1 |
0.8 |
2.3 |
0.5 |
0.3 |
|
n= |
1,373 |
924 |
397 |
21 |
60 |
13 |
8 |
|
|
The kindness and compassion shown by staff |
% |
49.4 |
34.7 |
11.2 |
1.3 |
2.9 |
0.3 |
0.2 |
|
n= |
1,407 |
955 |
308 |
36 |
77 |
8 |
5 |
|
|
The service they were meant to provide was completed |
% |
40.7 |
37.1 |
10.8 |
5.7 |
5.3 |
0.2 |
0.1 |
|
n= |
1,158 |
1,024 |
299 |
168 |
138 |
4 |
5 |
|
Note a: Asked of those who reported receiving the service.
Source: CHSP client survey.
Table A.41: Thinking about the most recent time you received a cleaning, laundry and other household chores service in your home or community from a local provider, how satisfied or dissatisfied were you with the following aspects?a
|
|
|
Very satisfied |
Satisfied |
Neither satisfied nor dissatisfied |
Dissatisfied |
Very dissatisfied |
Not sure |
Prefer not to answer |
|
The overall quality of the service provided |
% |
37.6 |
42.0 |
11.5 |
5.6 |
3.0 |
0.1 |
0.1 |
|
n= |
2,038 |
2,205 |
597 |
285 |
151 |
3 |
7 |
|
|
Alignment of the service to your care plan |
% |
34.4 |
43.9 |
13.6 |
5.0 |
2.6 |
0.4 |
0.2 |
|
n= |
1,871 |
2,292 |
706 |
251 |
136 |
20 |
10 |
|
|
The service provided met your needs |
% |
36.5 |
42.4 |
11.0 |
6.8 |
3.1 |
0.1 |
0.1 |
|
n= |
1,978 |
2,223 |
561 |
353 |
162 |
3 |
6 |
|
|
Staff arrived when they said they would |
% |
47.6 |
36.7 |
8.3 |
4.6 |
2.6 |
0.1 |
0.1 |
|
n= |
2,578 |
1,894 |
430 |
240 |
136 |
3 |
5 |
|
|
The professionalism of the service staff |
% |
48.4 |
36.6 |
9.8 |
3.2 |
1.9 |
0.1 |
0.1 |
|
n= |
2,623 |
1,914 |
486 |
165 |
90 |
3 |
5 |
|
|
How the staff communicated with you |
% |
50.4 |
37.8 |
7.3 |
2.5 |
1.8 |
0.1 |
0.1 |
|
n= |
2,729 |
1,948 |
374 |
133 |
95 |
3 |
4 |
|
|
The staff respected your cultural or personal identity |
% |
50.0 |
37.2 |
10.5 |
0.8 |
1.1 |
0.2 |
0.2 |
|
n= |
2,707 |
1,901 |
562 |
44 |
55 |
9 |
8 |
|
|
The kindness and compassion shown by staff |
% |
53.1 |
36.9 |
7.6 |
1.0 |
1.3 |
0.1 |
0.1 |
|
n= |
2,875 |
1,900 |
386 |
50 |
66 |
4 |
5 |
|
|
The service they were meant to provide was completed |
% |
37.9 |
43.1 |
10.9 |
5.5 |
2.5 |
0.1 |
0.1 |
|
n= |
2,043 |
2,278 |
545 |
275 |
133 |
5 |
7 |
|
Note a: Asked of those who reported receiving the service.
Source: CHSP client survey.
Table A.42: Thinking about the most recent time you received a aids to stay independent service in your home or community from a local provider, how satisfied or dissatisfied were you with the following aspects?a
|
|
|
Very satisfied |
Satisfied |
Neither satisfied nor dissatisfied |
Dissatisfied |
Very dissatisfied |
Not sure |
Prefer not to answer |
|
The overall quality of the service provided |
% |
39.4 |
40.3 |
12.4 |
3.9 |
3.4 |
0.4 |
0.2 |
|
n= |
679 |
666 |
206 |
64 |
56 |
6 |
4 |
|
|
Alignment of the service to your care plan |
% |
35.8 |
41.5 |
15.2 |
4.1 |
2.8 |
0.4 |
0.2 |
|
n= |
621 |
690 |
241 |
72 |
47 |
6 |
4 |
|
|
The service provided met your needs |
% |
37.7 |
40.8 |
12.8 |
4.2 |
3.9 |
0.3 |
0.2 |
|
n= |
657 |
676 |
202 |
73 |
64 |
4 |
5 |
|
|
Staff arrived when they said they would |
% |
45.2 |
37.9 |
11.6 |
2.3 |
2.3 |
0.5 |
0.2 |
|
n= |
773 |
622 |
191 |
44 |
39 |
7 |
5 |
|
|
The professionalism of the service staff |
% |
47.5 |
36.9 |
10.6 |
2.4 |
1.9 |
0.5 |
0.1 |
|
n= |
812 |
613 |
171 |
42 |
33 |
7 |
3 |
|
|
How the staff communicated with you |
% |
45.2 |
38.0 |
10.6 |
3.4 |
2.2 |
0.5 |
0.1 |
|
n= |
774 |
629 |
171 |
60 |
37 |
7 |
3 |
|
|
The staff respected your cultural or personal identity |
% |
46.5 |
36.2 |
14.4 |
0.8 |
1.3 |
0.6 |
0.2 |
|
n= |
791 |
604 |
235 |
15 |
23 |
9 |
4 |
|
|
The kindness and compassion shown by staff |
% |
48.9 |
36.2 |
11.3 |
1.3 |
1.7 |
0.4 |
0.1 |
|
n= |
835 |
600 |
183 |
25 |
29 |
6 |
3 |
|
|
The service they were meant to provide was completed |
% |
37.8 |
40.1 |
13.1 |
5.1 |
3.5 |
0.3 |
0.1 |
|
n= |
657 |
658 |
212 |
85 |
62 |
4 |
3 |
|
Note a: Asked of those who reported receiving the service.
Source: CHSP client survey.
Table A.43: Thinking about the most recent time you received a transport service in your home or community from a local provider, how satisfied or dissatisfied were you with the following aspects?a
|
|
|
Very satisfied |
Satisfied |
Neither satisfied nor dissatisfied |
Dissatisfied |
Very dissatisfied |
Not sure |
Prefer not to answer |
|
The overall quality of the service provided |
% |
48.8 |
35.8 |
9.5 |
3.6 |
1.8 |
0.2 |
0.3 |
|
n= |
833 |
563 |
151 |
57 |
32 |
4 |
6 |
|
|
Alignment of the service to your care plan |
% |
44.5 |
36.1 |
12.7 |
3.6 |
2.3 |
0.5 |
0.4 |
|
n= |
755 |
568 |
208 |
59 |
41 |
8 |
7 |
|
|
The service provided met your needs |
% |
47.2 |
36.1 |
9.2 |
4.9 |
2.0 |
0.2 |
0.3 |
|
n= |
798 |
571 |
154 |
76 |
37 |
4 |
6 |
|
|
Staff arrived when they said they would |
% |
51.0 |
33.2 |
10.5 |
2.7 |
1.9 |
0.4 |
0.3 |
|
n= |
854 |
526 |
173 |
48 |
33 |
7 |
5 |
|
|
The professionalism of the service staff |
% |
52.8 |
33.5 |
9.9 |
1.7 |
1.5 |
0.4 |
0.3 |
|
n= |
888 |
534 |
160 |
27 |
25 |
7 |
5 |
|
|
How the staff communicated with you |
% |
51.3 |
34.2 |
10.1 |
1.8 |
2.0 |
0.3 |
0.3 |
|
n= |
863 |
549 |
161 |
30 |
32 |
6 |
5 |
|
|
The staff respected your cultural or personal identity |
% |
49.7 |
34.9 |
12.8 |
0.4 |
1.3 |
0.5 |
0.3 |
|
n= |
836 |
551 |
214 |
9 |
21 |
9 |
6 |
|
|
The kindness and compassion shown by staff |
% |
54.7 |
32.3 |
10.1 |
0.8 |
1.4 |
0.5 |
0.3 |
|
n= |
916 |
513 |
166 |
15 |
23 |
8 |
5 |
|
|
The service they were meant to provide was completed |
% |
49.1 |
36.3 |
8.5 |
3.5 |
2.1 |
0.2 |
0.3 |
|
n= |
827 |
574 |
141 |
55 |
39 |
4 |
6 |
|
Note a: Asked of those who reported receiving the service.
Source: CHSP client survey.
Table A.44: Thinking about the most recent time you received a social outings service in your home or community from a local provider, how satisfied or dissatisfied were you with the following aspects?a
|
|
|
Very satisfied |
Satisfied |
Neither satisfied nor dissatisfied |
Dissatisfied |
Very dissatisfied |
Not sure |
Prefer not to answer |
|
The overall quality of the service provided |
% |
49.8 |
37.4 |
8.6 |
2.3 |
1.6 |
0.3 |
– |
|
n= |
443 |
318 |
83 |
17 |
14 |
3 |
0 |
|
|
Alignment of the service to your care plan |
% |
45.3 |
37.8 |
11.7 |
3.0 |
1.6 |
0.6 |
– |
|
n= |
406 |
320 |
108 |
25 |
13 |
6 |
0 |
|
|
The service provided met your needs |
% |
47.5 |
36.7 |
10.3 |
3.4 |
1.7 |
0.4 |
– |
|
n= |
424 |
312 |
93 |
29 |
16 |
4 |
0 |
|
|
Staff arrived when they said they would |
% |
51.0 |
35.7 |
9.2 |
2.1 |
1.2 |
0.6 |
0.3 |
|
n= |
458 |
301 |
82 |
18 |
11 |
6 |
2 |
|
|
The professionalism of the service staff |
% |
57.4 |
32.2 |
7.2 |
1.4 |
0.8 |
0.6 |
0.3 |
|
n= |
515 |
274 |
61 |
14 |
7 |
6 |
1 |
|
|
How the staff communicated with you |
% |
55.2 |
34.1 |
7.1 |
1.9 |
0.8 |
0.5 |
0.3 |
|
n= |
493 |
294 |
60 |
17 |
8 |
5 |
1 |
|
|
The staff respected your cultural or personal identity |
% |
54.5 |
34.3 |
8.8 |
0.6 |
1.0 |
0.6 |
0.3 |
|
n= |
486 |
290 |
82 |
6 |
7 |
6 |
1 |
|
|
The kindness and compassion shown by staff |
% |
59.8 |
31.5 |
6.1 |
1.0 |
0.8 |
0.6 |
0.3 |
|
n= |
534 |
269 |
52 |
9 |
7 |
6 |
1 |
|
|
The service they were meant to provide was completed |
% |
49.2 |
38.7 |
7.6 |
2.4 |
1.5 |
0.6 |
– |
|
n= |
439 |
326 |
75 |
20 |
13 |
5 |
0 |
|
Note a: Asked of those who reported receiving the service.
Source: CHSP client survey.
Table A.45: Are there any other types of support services that you would like to be able to receive in your home or community that you are not receiving at the moment?
|
Option |
n= |
Percentage (%) |
|
Yes |
5,762 |
57.4 |
|
No |
4,265 |
41.6 |
|
Not sure |
82 |
0.8 |
|
Prefer not to answer |
16 |
0.2 |
|
Total |
10,125 |
100 |
Source: CHSP client survey.
Table A.46: Other support services that clients would like to be able to receive in their home or community that they are not receiving at the momenta
|
Service |
n= |
Percentage of clients naming each service |
|
Cleaning / Domestic Assistance |
1,864 |
46.2 |
|
Gardening / Lawn Maintenance |
1,498 |
37.1 |
|
Meal Services |
390 |
9.7 |
|
Home Maintenance / Repairs |
1,511 |
37.4 |
|
Transport |
243 |
6.0 |
|
Social Support / Activities |
113 |
2.8 |
|
Health Services |
441 |
10.9 |
|
Safety / Equipment |
296 |
7.3 |
|
Total responses |
4,038 |
N/A |
Note a: Asked of those who would like other support services.
Source: CHSP client survey.
Table A.47: Has there ever been a time when you could not get an aged care service in your home or community that you needed?
|
Option |
n= |
Percentage (%) |
|
Yes |
5,131 |
50.5 |
|
No |
4,855 |
48.1 |
|
Not sure |
95 |
0.9 |
|
Prefer not to answer |
44 |
0.5 |
|
Total |
10,125 |
100 |
Source: CHSP client survey.
Table A.48: Which, if any, of the following were the reasons why you could not get the aged care service that you needed?a
|
Option |
n= |
Percentage of clients citing each reason |
|
Cost or financial barriers |
775 |
15.7 |
|
Local providers of that service were not available |
3,567 |
69.2 |
|
Local provider not accepting new clients |
2,256 |
44.8 |
|
Lack of access to transport |
385 |
7.7 |
|
Waiting for access to a Home Care Package |
1,551 |
31.7 |
|
Otherb |
1,199 |
23.2 |
|
Not sure |
35 |
0.7 |
|
Prefer not to answer |
17 |
0.4 |
|
Total responses |
5,131 |
N/A |
Note a: Asked of those who could not get an aged care service in their home or community that they needed.
Note b: This option provided the opportunity for respondents to give a free text response.
Source: CHSP client survey.
Table A.49: Thinking about your overall experience in the last six months, how satisfied or dissatisfied are you with the aged care services you have received in your home from a local provider through the Commonwealth Home Support Program?a
|
Option |
n= |
Percentage (%) |
|
Very satisfied |
2,597 |
28.2 |
|
Satisfied |
3,257 |
36.5 |
|
Neither satisfied nor dissatisfied |
1,499 |
17.1 |
|
Dissatisfied |
794 |
8.6 |
|
Very dissatisfied |
834 |
9.2 |
|
Not sure |
25 |
0.2 |
|
Prefer not to answer |
19 |
0.2 |
|
Total |
9,025 |
100 |
Note a: Asked of respondents receiving aged care services in their home or community or responding on behalf of someone who receives services.
Source: CHSP client survey.
Table A.50: Thinking about the aged care services that you have received in your home from a local provider through the Commonwealth Home Support Program in the last six months, to what extent has it changed your …?a
|
|
|
Improved a lot |
Improved a little |
No impact |
Worsened a little |
Worsened a lot |
Not sure |
Prefer not to answer |
|
Physical health |
% |
22.6 |
35.5 |
28.8 |
6.7 |
4.8 |
0.9 |
0.6 |
|
n= |
2,034 |
3,189 |
2,623 |
623 |
430 |
76 |
50 |
|
|
Emotional health |
% |
22.2 |
31.6 |
32.2 |
7.8 |
4.6 |
0.9 |
0.6 |
|
n= |
2,003 |
2,858 |
2,897 |
721 |
412 |
81 |
53 |
|
|
Mental health |
% |
20.8 |
29.6 |
36.0 |
7.3 |
4.7 |
1.0 |
0.6 |
|
n= |
1,884 |
2,663 |
3,246 |
676 |
420 |
85 |
51 |
|
|
Level of independence |
% |
20.9 |
33.2 |
35.7 |
5.8 |
3.5 |
0.6 |
0.4 |
|
n= |
1,882 |
2,980 |
3,243 |
528 |
297 |
60 |
35 |
|
|
Quality of life |
% |
28.0 |
37.8 |
21.8 |
6.8 |
4.1 |
0.9 |
0.6 |
|
n= |
2,538 |
3,382 |
1,986 |
633 |
360 |
75 |
51 |
|
|
Ability to stay living in your own home |
% |
29.5 |
30.1 |
32.4 |
4.4 |
2.6 |
0.6 |
0.4 |
|
n= |
2,626 |
2,698 |
2,982 |
397 |
226 |
61 |
35 |
|
|
Ability to participate in your community |
% |
12.2 |
20.0 |
58.9 |
4.4 |
3.4 |
0.6 |
0.5 |
|
n= |
1,091 |
1,793 |
5,351 |
399 |
289 |
60 |
42 |
|
|
Social connections |
% |
12.1 |
19.4 |
60.0 |
4.4 |
3.0 |
0.6 |
0.5 |
|
n= |
1,077 |
1,738 |
5,459 |
389 |
264 |
59 |
39 |
|
|
Ability to remain connected to your cultural or personal identity |
% |
12.0 |
15.0 |
66.5 |
2.8 |
2.3 |
0.7 |
0.6 |
|
n= |
1,071 |
1,318 |
6,074 |
245 |
199 |
71 |
47 |
|
Note a: Asked of respondents receiving aged care services in their home or community or responding on behalf of someone who receives services.
Source: CHSP client survey.
Table A.51: Are you of Aboriginal or Torres Strait Islander origin?
|
Option |
n= |
Percentage (%) |
|
Yes — Aboriginal |
330 |
1.9 |
|
Yes — Torres Strait Islander |
8 |
0.1 |
|
Yes — both |
13 |
0.1 |
|
No |
9,706 |
97.3 |
|
Not sure |
9 |
0.1 |
|
Prefer not to answer |
59 |
0.6 |
|
Total |
10,125 |
100 |
Source: CHSP client survey.
Table A.52: Thinking about your culture and connection, how much do you agree or disagree that the aged care services provided in your home and community in the last six months through the Commonwealth Home Support Program?a
|
|
Support my connection to family and kinship groups |
Support my connection to country |
Support my ability to participate in cultural practices or traditions |
|||
|
Option |
n= |
% |
n= |
% |
n= |
% |
|
Strongly agree |
29 |
9.9 |
34 |
11.2 |
29 |
9.4 |
|
Agree |
60 |
17.3 |
57 |
15.8 |
54 |
14.8 |
|
Neither agree nor disagree |
162 |
53.1 |
159 |
52.9 |
164 |
55.0 |
|
Disagree |
29 |
8.3 |
31 |
9.0 |
34 |
9.7 |
|
Strongly disagree |
34 |
11.4 |
33 |
11.2 |
33 |
11.1 |
|
Not sure |
0 |
– |
0 |
– |
0 |
– |
|
Prefer not to answer |
0 |
– |
0 |
– |
0 |
– |
|
Total respondents |
314 |
100 |
314 |
100 |
314 |
100 |
Note a: Asked of those who identified as Aboriginal or Torres Strait Islander.
Source: CHSP client survey.
Table A.53: Thinking about your experiences with the aged care services provided in your home and community through Commonwealth Home Support Program in the last six months, did you feel that your cultural or personal identity was respected and understood?a
|
Option |
n= |
Percentage (%) |
|
Yes, definitely |
5,147 |
57.2 |
|
Yes, somewhat |
2,187 |
24.6 |
|
No, not really |
880 |
9.5 |
|
No, not at all |
482 |
5.2 |
|
Not sure |
200 |
2.2 |
|
Prefer not to answer |
129 |
1.4 |
|
Total |
9,025 |
100 |
Note a: Asked of respondents receiving aged care services in their home or community or responding on behalf of someone who receives services.
Source: CHSP client survey.
Table A.54: Thinking about when you receive aged care services in your home through the Commonwealth Home Support Program, how comfortable or uncomfortable do you feel sharing your cultural or personal identity?a
|
Option |
n= |
Percentage (%) |
|
Very comfortable |
2,494 |
27.7 |
|
Comfortable |
2,681 |
30.4 |
|
Neither comfortable nor uncomfortable |
3,161 |
34.6 |
|
Uncomfortable |
234 |
2.5 |
|
Very uncomfortable |
287 |
3.1 |
|
Not sure |
72 |
0.8 |
|
Prefer not to answer |
96 |
1.0 |
|
Total |
9,025 |
100 |
Note a: Asked of respondents receiving aged care services in their home or community or responding on behalf of someone who receives services.
Source: CHSP client survey.
Table A.55: Do you have any suggestions for improving the Commonwealth Home Support Program?
|
Option |
n= |
Percentage (%) |
|
Yes |
5,387 |
53.2 |
|
No |
4,663 |
46.1 |
|
Not sure |
38 |
0.4 |
|
Prefer not to answer |
36 |
0.36 |
|
Total |
10,125 |
100 |
Source: CHSP client survey.
Table A.56: Suggestions for improvement to the Commonwealth Home Support Programa
|
Suggestion |
n= |
Percentage of clients making each suggestion |
|
Improved assessment process |
37 |
8.7 |
|
Shorter waiting times |
75 |
16.1 |
|
Improved communication and more support to navigate |
83 |
16.3 |
|
Availability of providers / services |
108 |
20.6 |
|
Consistency in staffing, contacts or service delivery |
28 |
5.2 |
|
More staff / employ more people |
38 |
8.2 |
|
Better / more trained staff |
33 |
8.0 |
|
Better / increased funding |
35 |
6.9 |
|
Reduce costs for services |
27 |
6.0 |
|
Better follow up and oversight |
44 |
8.4 |
|
Tailored services to individual needs |
30 |
5.7 |
|
More service options |
36 |
8.2 |
|
Simplify the process |
59 |
12.4 |
|
Provide help |
41 |
7.5 |
|
Other |
50 |
10.0 |
|
Don’t know |
1 |
0.3 |
|
Prefer not to say |
4 |
0.7 |
|
Total number of respondents |
500 |
N/A |
Note a: This analysis is based on 500 randomly selected respondents responding to the question.
Source: CHSP client survey.
Table A.57: Which age group do you fall into?
|
Option |
n= |
Percentage (%) |
|
18–44 years |
1 |
0.0 |
|
45–54 years |
38 |
0.4 |
|
55–64 years |
110 |
1.0 |
|
65–69 years |
1,049 |
9.4 |
|
70–74 years |
1,981 |
18.4 |
|
75–79 years |
2,945 |
28.3 |
|
80–84 years |
2,387 |
23.3 |
|
85–89 years |
1,174 |
13.9 |
|
90 or more years |
434 |
5.3 |
|
Not sure |
1 |
0.0 |
|
Prefer not to answer |
5 |
0.1 |
|
Total |
10,125 |
100 |
Source: CHSP client survey.
Table A.58: Which state do you currently live in?
|
Statea |
n= |
Percentage (%) |
|
NSW |
2,740 |
32.0 |
|
VIC |
2,235 |
22.1 |
|
QLD |
2,753 |
25.6 |
|
SA |
1,029 |
8.7 |
|
WA |
829 |
7.3 |
|
TAS |
226 |
1.9 |
|
NT |
34 |
0.3 |
|
ACT |
278 |
2.1 |
|
Not sure |
0 |
– |
|
Prefer not to answer |
0 |
– |
|
Total |
10,124 |
100 |
Note a: To derive state location data. respondents were also asked for postcode or suburb. Respondents were able to enter postcodes as an open text question (assisted by a lookup list). In cases of invalid or mistyped entries, it is not possible to match the respondent to a state if the postcode does not appear in the concordance file for geographic locations. This missing record is one such case.
Source: CHSP client survey.
Table A.59: Location of clients by capital city/rest of state
|
Location |
n= |
Percentage (%) |
|
Greater Sydney |
1,243 |
16.4 |
|
Rest of NSW |
1,355 |
13.9 |
|
Greater Melbourne |
1,426 |
15.1 |
|
Rest of Vic. |
718 |
6.1 |
|
Greater Brisbane |
1,197 |
11.7 |
|
Rest of Qld |
1,405 |
12.5 |
|
Greater Adelaide |
747 |
6.4 |
|
Rest of SA |
239 |
1.9 |
|
Greater Perth |
623 |
5.7 |
|
Rest of WA |
173 |
1.3 |
|
Greater Hobart |
84 |
0.7 |
|
Rest of Tas. |
137 |
1.1 |
|
Greater Darwin |
26 |
0.3 |
|
Rest of NT |
6 |
0.1 |
|
Australian Capital Territory |
265 |
2.0 |
|
Unable to establish |
481 |
4.7 |
|
Total |
10,125 |
100 |
Source: CHSP client survey.
Table A.60: In which country were you born?
|
Country |
n= |
Percentage (%) |
|
Australia |
7,263 |
64.9 |
|
England |
851 |
7.6 |
|
New Zealand |
242 |
3.4 |
|
United Kingdom, Channels Islands and Isle of Man, nfd |
202 |
1.7 |
|
Scotland |
137 |
1.2 |
|
Germany |
101 |
1.4 |
|
Italy |
99 |
1.6 |
|
Netherlands |
86 |
1.2 |
|
India |
70 |
1.1 |
|
United States of America |
65 |
0.5 |
|
South Africa |
65 |
1.0 |
|
China (excludes SARs and Taiwan) |
61 |
1.2 |
|
Greece |
58 |
1.0 |
|
Sri Lanka |
58 |
1.0 |
|
Other |
709 |
10.4 |
|
Don’t know |
58 |
0.7 |
|
Total |
10,125 |
100 |
Source: CHSP client survey.
Table A.61: Do you use a language other than English at home?
|
Option |
n= |
Percentage (%) |
|
Yes |
827 |
12.4 |
|
No |
9,291 |
87.6 |
|
Not sure |
1 |
0.0 |
|
Prefer not to say |
6 |
0.1 |
|
Total |
10,125 |
100 |
Source: CHSP client survey.
Table A.62: Which language other than English do you use at home?
|
Language |
n= |
Percentage (%) |
|
English |
118 |
9.2 |
|
Greek |
69 |
9.5 |
|
Italian |
61 |
8.4 |
|
Yue (Cantonese) |
47 |
7.1 |
|
Mandarin |
34 |
5.1 |
|
Refused |
30 |
2.7 |
|
German |
28 |
3.4 |
|
Spanish |
26 |
3.6 |
|
Chinese Languages, nfd |
22 |
2.7 |
|
Dutch |
19 |
2.1 |
|
Arabic |
19 |
2.9 |
|
French |
16 |
2.0 |
|
Polish |
16 |
1.8 |
|
Sinhalese |
16 |
2.4 |
|
Tamil |
15 |
1.9 |
|
Vietnamese |
15 |
2.4 |
|
Tagalog |
15 |
1.9 |
|
Croatian |
13 |
1.8 |
|
Hindi |
13 |
2.0 |
|
Maltese |
13 |
1.9 |
|
Filipino |
12 |
1.7 |
|
Russian |
11 |
1.5 |
|
Auslan |
11 |
0.8 |
|
Macedonian |
8 |
0.8 |
|
Hungarian |
6 |
0.7 |
|
Turkish |
6 |
0.8 |
|
Danish |
5 |
0.7 |
|
Persian (excluding Dari) |
5 |
0.8 |
|
Fiji Hindi |
5 |
0.7 |
|
Punjabi |
5 |
0.5 |
|
Korean |
5 |
0.7 |
|
Min Nan (Teochew) |
5 |
0.5 |
|
Other |
90 |
10.4 |
|
Don’t know |
48 |
4.4 |
|
Total |
827 |
100 |
Source: CHSP client survey.
Table A.63: Which of the following best describes where you currently live?
|
Option |
n= |
Percentage (%) |
|
In my own home (e.g. house, townhouse, or apartment) |
8,125 |
80.0 |
|
With family or friends in their home |
436 |
4.8 |
|
In a retirement village or independent living unit |
1,349 |
13.0 |
|
In residential aged care (e.g. nursing home or hostel) |
113 |
1.3 |
|
In a temporary or emergency accommodation (e.g. shelter, caravan, motel) |
46 |
0.4 |
|
In a hospital, rehabilitation centre, or similar facility |
9 |
0.1 |
|
Something elsea |
30 |
0.3 |
|
I don’t have a place of residence |
9 |
0.1 |
|
Not sure |
2 |
0.0 |
|
Prefer not to answer |
6 |
0.1 |
|
Total |
10,125 |
100 |
Note a: This option provided the opportunity for respondents to give a free text response.
Source: CHSP client survey.
Table A.64: Which of the following describes your household?a
|
Option |
n= |
Percentage (%) |
|
I live alone |
3,973 |
36.3 |
|
I live with my partner / spouse |
5,306 |
55.2 |
|
I live with my children |
570 |
6.1 |
|
I live with other relatives |
189 |
1.9 |
|
I live with other people who are not related to me |
219 |
2.0 |
|
Not sure |
3 |
0.0 |
|
Prefer not to say |
26 |
0.3 |
|
Total responses |
10,286 b |
100 |
|
Total respondents |
10,116 |
N/A |
Note a: Asked of those who have a place of residence.
Note b: Question allowed multiple responses.
Source: CHSP client survey.
Table A.65: Which of the following describes your situation?
|
Option |
I have children or other relatives who help me with daily living |
I have friends or neighbours who help me with daily living |
||
|
|
n= |
% |
n= |
% |
|
Always |
1,416 |
15.2 |
356 |
3.4 |
|
Sometimes |
4,265 |
42.7 |
3,375 |
33.1 |
|
Never |
4,415 |
41.9 |
6,322 |
62.8 |
|
Not sure |
1 |
0.0 |
19 |
0.2 |
|
Prefer not to answer |
28 |
0.3 |
53 |
0.6 |
|
Total |
10,125 |
100 |
10,125 |
100 |
Source: CHSP client survey.
Table A.66: Which of the following options best describes your access to regular transport?
|
Option |
n= |
Percentage (%) |
|
I have my own car |
6,480 |
61.6 |
|
I share a car with someone else |
552 |
5.5 |
|
Someone regularly drives me where I need to go |
1,718 |
18.3 |
|
I use community transport, taxis, or rideshare services |
612 |
6.4 |
|
I use public transport |
418 |
4.5 |
|
I do not have regular access to transport |
327 |
3.6 |
|
Not sure |
3 |
0.0 |
|
Prefer not to answer |
15 |
0.2 |
|
Total |
10,125 |
100 |
Source: CHSP client survey.
Table A.67: What is the highest year of primary or secondary school you have completed?
|
Option |
n= |
Percentage (%) |
|
Year 12 or equivalent |
5,129 |
51.0 |
|
Year 11 or equivalent |
908 |
8.4 |
|
Year 10 or equivalent |
2,747 |
26.3 |
|
Year 9 or equivalent |
703 |
6.9 |
|
Year 8 or below |
534 |
6.0 |
|
Did not go to school |
40 |
0.7 |
|
Not sure |
14 |
0.2 |
|
Prefer not to answer |
50 |
0.5 |
|
Total |
10,125 |
100 |
Source: CHSP client survey.
Table A.68: What is the level of the highest educational qualification you have completed, if any?
|
|
n= |
Percentage (%) |
|
Have not completed a qualification |
3,495 |
35.4 |
|
Postgraduate Degree Level (include Master Degree, Doctoral Degree, other postgraduate degree) |
955 |
9.3 |
|
Graduate Diploma and/or Graduate Certificate Level |
1,049 |
10.0 |
|
Bachelor Degree Level |
1,392 |
13.7 |
|
Advanced Diploma and/or Diploma Level |
1,014 |
9.8 |
|
Certificate III and/or IV Level |
1,352 |
13.0 |
|
Certificate I and/or II Level |
241 |
2.4 |
|
Other (please specify)a |
451 |
4.7 |
|
Not sure |
58 |
0.6 |
|
Prefer not to answer |
118 |
1.2 |
|
Total |
10,125 |
100 |
Note a: This option provided the opportunity for respondents to give a free text response.
Source: CHSP client survey.
Table A.69: Before tax or other deductions, what is your personal total annual income?
|
|
n= |
Percentage (%) |
|
$1 – $33,799 per year ($1 – $649 per week) |
4,911 |
49.0 |
|
$33,800 – $41,599 per year ($650 – $799 per week) |
1,528 |
14.9 |
|
$41,600 – $51,999 per year ($800 – $999 per week) |
1,050 |
10.1 |
|
$52,000 – $77,999 per year ($1,000 – $1,499 per week |
837 |
8.0 |
|
$78,000 – $90,999 per year ($1,500 – $1,749 per week) |
230 |
2.1 |
|
$91,000 or more per year ($1,750 or more per week) |
190 |
1.8 |
|
$0 or nil income |
514 |
5.4 |
|
Negative income |
293 |
3.1 |
|
Not sure |
130 |
1.3 |
|
Prefer not to answer |
442 |
4.3 |
|
Total |
10,125 |
100 |
Source: CHSP client survey.
Table A.70: In general, would you say that your health is …?
|
|
n= |
Percentage (%) |
|
Excellent |
121 |
1.1 |
|
Very good |
1,127 |
10.9 |
|
Good |
2,826 |
27.6 |
|
Fair |
4,218 |
41.9 |
|
Poor |
1,827 |
18.4 |
|
Not sure |
1 |
0.0 |
|
Prefer not to answer |
5 |
0.1 |
|
Total |
10,125 |
100 |
Source: CHSP client survey.
Table A.71: Do you have a disability, health condition, or injury that has lasted or is likely to last 6 months or more?
|
|
n= |
Percentage (%) |
|
Yes |
8,585 |
84.0 |
|
No |
1,506 |
15.6 |
|
Not sure |
11 |
0.1 |
|
Prefer not to answer |
23 |
0.3 |
|
Total |
10,125 |
100 |
Source: CHSP client survey.
Table A.72: How do you describe your gender?
|
|
n= |
Percentage (%) |
|
Man or male |
4,049 |
40.1 |
|
Woman or female |
6,038 |
59.5 |
|
Non-binary |
5 |
0.0 |
|
I use a different term |
3 |
0.0 |
|
Not sure |
1 |
0.0 |
|
Prefer not to answer |
29 |
0.3 |
|
Total |
10,125 |
100 |
Source: CHSP client survey.
Table A.73: What was your sex recorded at birth?
|
|
n= |
Percentage (%) |
|
Male |
4,035 |
40.0 |
|
Female |
6,056 |
59.7 |
|
Another term |
2 |
0.0 |
|
Not sure |
1 |
0.0 |
|
Prefer not to answer |
31 |
0.3 |
|
Total |
10,125 |
100 |
Source: CHSP client survey.
Table A.74: How do you describe your sexual orientation?
|
|
n= |
Percentage (%) |
|
Heterosexual or straight |
9,383 |
92.7 |
|
Gay |
78 |
0.7 |
|
Lesbian |
54 |
0.5 |
|
Bisexual |
63 |
0.6 |
|
Asexual |
40 |
0.4 |
|
Pansexual |
4 |
0.0 |
|
Queer |
5 |
0.0 |
|
I use a different term |
13 |
0.1 |
|
Not sure |
27 |
0.4 |
|
Prefer not to answer |
458 |
4.7 |
|
Total |
10,125 |
100 |
Source: CHSP client survey.
Appendix 7 Public contributions to the audit
1. The ANAO received 59 public submissions to the audit.
2. The feedback received through the public contributions are presented throughout the audit report. Table A.75 provides a thematic summary of the feedback received.
Table A.75: Citizen contribution themes
|
Access and barriers |
Capacity |
Communication |
Compliance and administration burden |
Cultural |
Funding |
Objectives |
Other |
Reforms |
Service delivery |
Workforce |
Key:
Low frequency
Medium frequency
High frequency
Source: ANAO analysis of citizen contributions
Appendix 8 Commonwealth Home Support Program program logic
Figure A.4: Program Logic for the Commonwealth Home Support Program, 2023
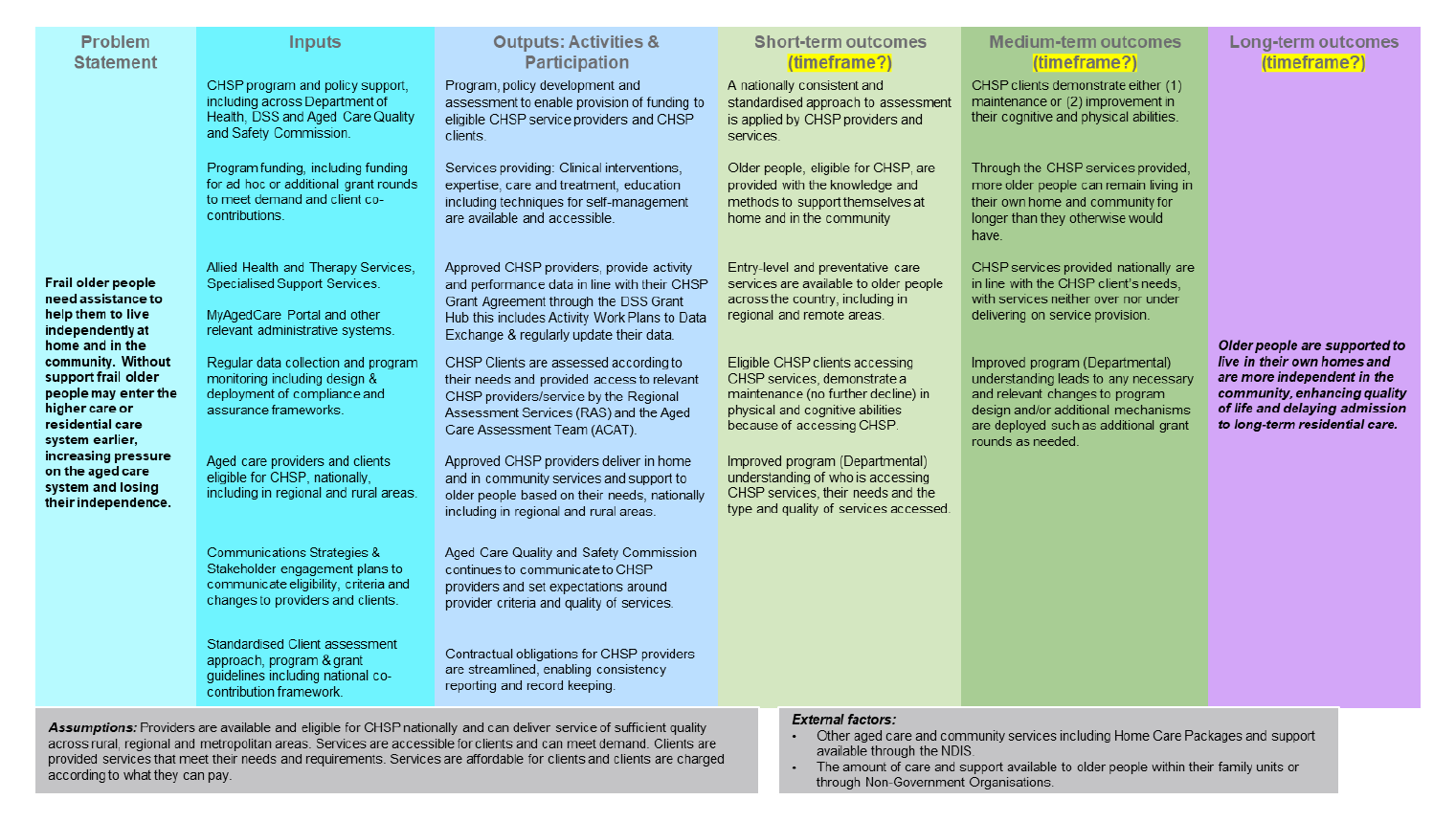
Source: Department of Health, Disability and Ageing.
Footnotes
1 Department of Health, Disability and Ageing, Commonwealth Home Support Program — Program Manual 2025–27 — Effective 1 November 2025, DHDA, Canberra, 2025 p. 8, available from https://www.health.gov.au/resources/publications/commonwealth-home-support-program-chsp- 2025-27-manual-from-1-november-2025?language=en [accessed 17 November 2025].
2 ibid., pp. 10–11.
3 Commonwealth of Australia, Administrative Arrangements Order, Department of the Prime Minister and Cabinet, Canberra, 13 May 2025, available from https://www.pmc.gov.au/resources/aao-13-may-2025 [accessed 1 December 2025].
4 Department of Health, Disability and Ageing, Annual Report 2024–25, 2025, DHDA, Canberra, p. 157, available from https://www.health.gov.au/resources/publications/department-of-health-disability-and-ageing-2024-25-annual-report?language=en [accessed 1 December 2025].
5 The System Governor oversees the aged care system, supporting fair access, service continuity, and quality care through policy, education, reporting, and system-wide stewardship.
Department of Health, Disability and Ageing, Guide to Aged Care Law — The System Governor, DHDA, Canberra, available from https://www.health.gov.au/resources/publications/guide-to-aged-care-law/chapter-5-governance-of-the-aged-care-system/the-system-governor?language=en [accessed 11 February 2026].
6 Department of Health, Disability and Ageing, About aged care, DHDA, Canberra, 2025, available from https://www.health.gov.au/topics/aged-care/about-aged-care [accessed 22 October 2025].
7 Commonwealth of Australia, Administrative Arrangements Order.
8 Department of Health, Disability and Ageing, Annual Report 2024–25, 2025, p. 157.
9 Aged Care Act, 2024 (Cth), section 338.
10 Department of Health, Disability and Ageing, About the Commonwealth Home Support Program (CHSP) [Internet], DHDA, Canberra, 2025, available from https://www.health.gov.au/our-work/chsp/about [accessed 5 November 2025].
11 Home Care Packages were designed for older Australians living at home with more complex needs, that went beyond what CHSP could provide. Packages provided a coordinated mix of care and services that could include help with household tasks, aids and equipment, minor home modifications, personal care and clinical care.
12 The Short-Term Restorative Care Program provided tailored services and support for up to eight weeks to help older people continue to live at home rather than go into long-term care. Services included occupational therapy, physiotherapy, nursing support, personal care, technology to help with day-to-day activities and minor home modifications.
13 Four programs were consolidated to form the CHSP: Commonwealth Home and Community Care; National Respite for Carers Program; Day Therapy Centres; and Assistance with Care and Housing for the Aged.
14 Department of Health, Disability and Ageing, Commonwealth Home Support Program, Program Manual 2025–27 — Effective 1 November 2025, DHDA, Canberra, 2025, pp. 10–11, available from https://www.health.gov.au/resources/publications/commonwealth-home-support-program-chsp- 2025-27-manual-from-1-november-2025?language=en [accessed 13 November 2025].
15 Department of Health, Disability and Ageing, About the Commonwealth Home Support Program (CHSP) [Internet], DHDA, Canberra, 2025, available from https://www.health.gov.au/our-work/chsp/about [accessed 5 November 2025].
16 The service type ‘sector support and development’ aims to increase provider capability and improve quality of service delivery through activities targeted in part at CHSP providers.
17 The Commonwealth Grants Rules and Principles state that one off ad hoc grants are determined on a proper use and value with relevant money basis, and usually by ministerial decision.
18 Demand-driven or ‘first-in first-served’ grant processes refer to where applications that satisfy stated eligibility criteria receive funding, up to the limit of available appropriations and subject to revision, suspension or abolition of the grant opportunity.
19 The Commonwealth Grants Rules and Principles define closed non-competitive grants as those, for example, where applicants are invited by the entity to submit applications or provide a proposal for a particular grant, and targeted competitive grants as open to a small number of potential grantees based on the specialised requirements of the grant activity under consideration.
20 Department of Health, Disability and Ageing, Annual Report 2024–25, p. 188.
People receiving CHSP services may be asked to contribute towards the cost of the services under the National CHSP Client Contribution Framework. Contributions are not means-tested.
Department of Health, Disability and Ageing, Appendix E — CHSP National Unit Price Ranges and Guide to the National CHSP Client Contribution Framework, DHDA, Canberra, 2025, pp. 2-4, available from https://www.health.gov.au/resources/publications/commonwealth-home-support-program-chsp- 2025-27-manual-from-1-november-2025?language=en [accessed 16 October 2025].
21 The Aged Care Act 2024 introduced new eligibility requirements from 1 November 2025. Frail older people or prematurely aged people aged 50 years and over (45 years and over for Aboriginal or Torres Strait Islander people) on low income and homeless or at risk of homelessness; or living with hoarding behaviour or in a squalid environment and at risk of homelessness or unable to receive the aged care services they need, were no longer eligible for CHSP services.
22 The Home Support Operations Branch within the Access and Home Support Division and Ageing and Aged Care Group of DHDA has primary responsibility for the management of the CHSP.
23 Aged Care Quality and Safety Commission, Quality Standards, ACQSC, Canberra, available from https://www.agedcarequality.gov.au/providers/quality-standards [accessed 24 February 2026].
24 One of three primary functions of the Aged Care Quality and Safety Commissioner is to protect and enhance the safety, health, wellbeing and quality of life of aged care recipients.
25 Royal Commission into Aged Care Quality and Safety, Final Report: Care, Dignity and Respect. Volume 1 — Summary and recommendations, Royal Commission, Adelaide, 2021, p. 6. The Australian Government’s response to the final report, May 2021, is available from https://www.health.gov.au/sites/default/files/documents/2021/05/australian-government-response-to-the-final-report-of-the-royal-commission-into-aged-care-quality-and-safety.pdf [accessed 17 January 2025].
26 See recommendations 1, 5, 25, 27, 31, 33, 35, 36, 111, 118, 119, 123 and 124.Royal Commission, Final Report — volume 1, available from: https://www.royalcommission.gov.au/system/files/2021-03/final-report-recommendations.pdf [accessed 28 November 2024].
27 Department of Health, Budget 2021 — Health Portfolio 2021–22 Budget Stakeholder Pack, DoH, Canberra, 2021, pp. 104 and 143, available at https://parlinfo.aph.gov.au/parlInfo/search/display/display.w3p;query=Id%3A%22media%2Fpressrel%2F7954999%22 [accessed 14 November 2025].
28 Minister for Aged Care, ‘Support at home to be rolled out in two stages’, media release, 28 November 2023, available from https://parlinfo.aph.gov.au/parlInfo/search/display/display.w3p;query=Id%3A%22media% 2Fpressrel%2F9492209%22 [accessed 14 November 2025].
29 Standard monthly payments are calculated by DHDA as the total value of a provider’s grant agreement divided by 12. Sector support development providers receive upfront quarterly payments.
30 Aged Care Act 2024, section 5, available from https://www.legislation.gov.au/C2024A00104/latest/text [accessed 28 October 2025].
31 Department of Health, Disability and Ageing, Commonwealth Home Support Program Manual, 2025–27 DHDA, Canberra, November 2025, p. 9, available from https://www.health.gov.au/sites/default/files/2025-12/chsp_ 2025-27_manual_1_november_2025_updated_end_november_2025_version_2.pdf [accessed 28 October 2025].
32 Australian Public Service Academy, Delivering Great Policy, APSA, Canberra, available from https://www.apsacademy.gov.au/aps-craft/strategy-policy-evaluation/delivering-great-policy [accessed 11 September 2025].
33 Department of Health, Disability and Ageing, Commonwealth Home Support Program (CHSP) 2025–27 Manual, DHDA, Canberra, 1 November 2025, Section 12.5, p. 91, available from https://www.health.gov.au/resources/publications/commonwealth-home-support-program-chsp- 2025-27-manual-from-1-november-2025?language=en [accessed on 5 May 2026].
34 A similar explanation of the CHSP Planning Framework was included in versions of the CHSP Manual since 2022–23.
35 Older Persons Advocacy Network, Reports, OPAN, available from https://opan.org.au/information/publications-and-reports/reports/ [accessed 28 October 2025].
36 Australian Government, Care Sector Demand Map, Department of Social Services, Canberra, available from https://caresectordemandmap.dss.gov.au/ [accessed 9 July 2025]. As at October 2025, the data was for 2023–24.
37 Australian Institute of Health and Welfare, GEN Aged Care Data, AIHW, Canberra, available from https://www.gen-agedcaredata.gov.au/ [accessed 28 October 2025].
38 Australian Institute of Health and Welfare, CHSP aged care services, AIHW, Canberra, available from https://www.gen-agedcaredata.gov.au/resources/dashboards/commonwealth-home-support-programme-aged-care-services [accessed 2 November 2025].
39 Aged care services in Australia are funded and delivered in regions called Aged Care Planning Regions, of which there are 73 across Australia.
Department of Health, Disability and Ageing, 2018 Aged Care Planning Region maps, DHDA, Canberra, available from https://www.health.gov.au/resources/collections/2018-aged-care-planning-region-maps [accessed 30 June 2025].)
40 My Aged Care is a website and contact centre that facilitates the dissemination of information on aged care services and provides a platform for Australians to apply for an aged care assessment, available from https://www.myagedcare.gov.au/ [accessed 17 October 2025].
41 The Aged Care Data Warehouse is the central repository for current and historical CHSP and other aged care program data, and includes data about aged care providers, aged care services, participants, payments, and other administrative data.
42 Senate Standing Committees on Community Affairs, Australian Parliament, Aged care service delivery (2025), paragraph 4.3, available from https://www.aph.gov.au/Parliamentary_Business/Committees/Senate /Community_Affairs/Agedcareservice/Report [accessed 26 February 2026].
43 Two outcomes of an aged care assessment can be a service referral to CHSP or a general recommendation, which relates to a type of support that is non-Commonwealth funded or where the referral is made outside of the My Aged Care portal.
Department of Health, Disability and Ageing, My Aged Care Assessment Manual, DHDA, Canberra, 2025, p. 300, available from https://www.health.gov.au/sites/default/files/2025-10/my-aged-care-assessment-manual.pdf [accessed 2 December 2025].
44 Australian Institute of Health and Welfare, 2023 Aged Care Provider Workforce Survey Report, AIHW, Canberra, 2024, p. 1, available from https://www.gen-agedcaredata.gov.au/getmedia/aa6c9983-5ee1-42c2-a7a8-183d76fad46b/2023_ACPWS_Report [accessed 4 November 2025].
45 Qlik Sense is a business intelligence platform that supports real time monitoring and data visualisation (see https://www.qlik.com/us [accessed 17 October 2025]). IBM Cognos is a reporting and data visualisation tool, (see https://www.ibm.com/products/cognos-analytics [accessed 17 October 2025]).
46 Australian Government, Care Sector Demand Map.
47 The Assistive Technology and Home Modifications scheme provides Support at Home program participants with separate funding for assistive technology and home modifications, without needing to save up funds from their quarterly budgets for ongoing services.
Department of Health, Disability and Ageing, Assistive Technology and Home Modifications (AT-HM) scheme [Internet], DHDA, Canberra, 2026, available from https://www.health.gov.au/our-work/support-at-home/delivering-services-for-support-at-home/assistive-technology-and-home-modifications-at-hm-scheme?language=en [accessed 24 February 2026].
48 The Modified Monash Model defines whether a location is metropolitan, rural, remote or very remote.
Department of Health, Disability and Ageing, Modified Monash Model [Internet], DHDA, Canberra, available from https://www.health.gov.au/topics/rural-health-workforce/classifications/mmm [accessed 17 September 2025].
49 Statistical Area Level 2 is a geographic unit derived from postcodes used by the Australian Bureau of Statistics in analysis of population and housing statistics. They are a medium-sized statistical geography, the purpose of which is to represent a community that interacts together socially and economically. There are 2,473 Statistical Area Level 2 covering the whole of Australia without gaps or overlaps.
Australian Bureau of Statistics, Statistical Area Level 2, Australian Statistical Geography Standard (ASGS) Edition 3, ABS, Canberra, available from https://www.abs.gov.au/statistics/standards/australian-statistical-geography-standard-asgs-edition-3/jul2021-jun2026/main-structure-and-greater-capital-city-statistical-areas/statistical-area-level-2 [accessed 28 October 2025].
50 DHDA administers specialist programs designed to cater for thin market service delivery such as the Multi-Purpose Service Program (MPSP) and the National Aboriginal and Torres Strait Islander Flexible Aged Care Program (NATSIFACP). These programs operate in a similar manner to CHSP and are funded using Commonwealth grants.
Department of Health, Disability and Ageing, Multi-Purpose Services (MPS) Program, DHDA, Canberra, available from https://www.health.gov.au/our-work/multi-purpose-services-mps-program [accessed 4 August 2025].
Department of Health, Disability and Ageing, National Aboriginal and Torres Strait Islander Flexible Aged Care Program, DHDA, Canberra, available from https://www.health.gov.au/our-work/national-aboriginal-and-torres-strait-islander-flexible-aged-care-program [accessed 4 August 2025].
51 Australian Bureau of Statistics, Disability, Ageing and Carers, Australia: Summary of Findings, ABS, Canberra, 2024, available from https://www.abs.gov.au/statistics/health/disability/disability-ageing-and-carers-australia-summary-findings/latest-release#older-people [accessed 19 January 2026].
52 Department of Health, Disability and Ageing, Annual Report 2024-25, p. 124.
53 Department of Health, Disability and Ageing, Financial Report on the Aged Care Sector 2023-24, DHDA, Canberra, 2025, available from https://www.health.gov.au/sites/default/files/2025-07/financial-report-on-the-australian-aged-care-sector-2023-24.pdf [accessed 23 July 2025].
54 G Meagher, Supplementary report on workforce and work value issues in Australian home care for older people, Macquarie University, Sydney, 2021, available from https://researchers.mq.edu.au/en/publications/supplementary-report-on-workforce-and-work-value-issues-in-austra/ [accessed 29 October 2025].
D Romano, C Littleton, F O’Reilly, M Kennedy, J Bender J, W Harding, Ageing in place, Torrens University, 2024, available from https://cdn.intelligencebank.com/au/share/RyzZ/kYPzN/9r6dV/original/Ageing-in-place-White-Paper-CHSD [accessed 29 October 2025].
55 The Aged Care Workforce Committee is made up of senior executives of DHDA, DSS and other government entities, unions, older persons’ advocacy organisations and large aged care providers.
56 KPMG Australia, Aged care sector analysis and report 2025, 2025, KPMG, available from https://kpmg.com/au/en/insights/industry/aged-care-market-analysis.html [accessed 21 October 2025].
57 Australian Government Department of Health and Aged Care, ‘New Aged Care Act and Support at Home program update’ [video], DoHAC, Canberra, 28 November 2023, available from https://www.youtube.com/watch?v=1goSJs8MEC0,[accessed 13 June 2025].
58 Australian Government, My Aged Care, available from https://www.myagedcare.gov.au/ [accessed 12 June 2025].
59 Department of Health, Disability and Ageing, My Aged Care Assessment Manual, DHDA, Canberra, November 2025, available from https://www.health.gov.au/resources/publications/my-aged-care-assessment-manual?language=en [accessed 2 December 2025].
60 DHDA advised the ANAO in November 2025 that its estimate was based on anecdotal reporting from the subset of CHSP providers that completed the 2025–27 CHSP extension stakeholder survey.
61 DHDA identified a high priority group (tranche 1), comprised of 37,000 people, for focused efforts to encourage registration and assessment. Tranche 1 was identified as having a high proportion of Aboriginal and Torres Strait Islander people and people from culturally and linguistically diverse backgrounds. Another 76,000 people received episodic services (based on service use in a six-month period in 2023–24).
62 The ANAO estimates that the cost of providing services to unregistered clients in 2024–25 was $448 million (based on DHDA’s estimate as at June 2025 of $3,996 average expenditure for each CHSP client).
63 Productivity Commission, Report on Government Services, 14 Aged Care Services, PC, Canberra, 2025, available from https://www.pc.gov.au/ongoing/report-on-government-services/2025/community-services/aged-care-services/ [accessed 29 October 2025].
64 Department of Health, Disability and Ageing, Annual Report 2024-25, p. 111
Allocated priority timeframes are: for high priority assessments, within 10 calendar days; for medium priority assessments, within 14 days; and for low priority assessments, within 21 calendar days. Between 2017–18 and 2024–25, for all aged care assessments, elapsed days at the 50th and 90th percentile and number of completed assessments increased, particularly at the 90th percentile.
65 High priority – 10 calendar days, medium priority – 14 calendar days, low priority – 21 calendar days.
Department of Health, Disability and Ageing, My Aged Care Assessment Manual, Canberra, 2026, p. 83, available from https://www.health.gov.au/sites/default/files/2026-03/my-aged-care-assessment-manual.pdf [accessed 15 April 2026].
66 The National Priority System determines the order in which eligible clients are assigned a Home Care Package and the package release process (the number and type of packages that can be assigned to clients in the queue).
67 Aged Care Act 2024, Part 1 — Preliminary, Section 5, available from https://www.legislation.gov.au/C2024A00104/latest/text [accessed 28 October 2025].
68 Australian Public Service Commission, Partnerships and engagement [Internet], APSC, Canberra, n.d., available from https://www.apsc.gov.au/initiatives-and-programs/workforce-information/research-analysis-and-publications/state-service/state-service-report-2023-24/fit-future/partnerships-and-engagement [accessed 8 September 2025]. The Secretary’s Board is comprised of the heads of Australian Government departments and under the Public Service Act 1999 has responsibility for stewardship of the Australian Public Service.
69 APS Reform Office, Good Practice Guidance — Charter of Partnerships and Engagement, APS Reforms, 2024, pp. 2–3.
70 Public Governance, Performance and Accountability Act 2013 (Cth), section 16.
71 Department of Finance, Commonwealth Risk Management Policy [Internet], Finance, updated 2022, available from https://www.finance.gov.au/government/comcover/risk-services/management/commonwealth-risk-management-policy [accessed 25 September 2025].
72 Department of Finance, Australian Government Grants Framework, Finance, Canberra, available from https://www.finance.gov.au/government/commonwealth-grants/australian-government-grants-framework and from https://www.legislation.gov.au/F2024L00854/latest/text [accessed 3 November 2025].
73 Department of Health, Disability and Ageing, Stakeholder engagement framework, DHDA, Canberra, 2017, available from https://www.health.gov.au/resources/publications/stakeholder-engagement-framework?language=en [accessed 2 January 2026].
74 DHDA established two pilot programs to support the transition of transport services and meal services to the Support at Home program.
Auditor-General Report No. 37 2024–25, Administration of the Future Fit Program, ANAO, Canberra, 2025, available from https://www.anao.gov.au/work/performance-audit/administration-of-the-future-fit-program.
75 Examples in 2024–25 include consultations on: a national registration scheme to support personal care workers in aged care; establishment of a National Aged Care Mandatory Quality Indicator Program for in home aged care services; and local government aged care services provision.
76 Sector support and development aims to increase CHSP provider capability and improve quality of service delivery.
77 As at December 2025, the Forum had met four times.
78 The ANAO did not assess the December 2025 MOU.
79 The program assurance group also discusses the Disability Support for Older Australians (DSOA) program, which was established for people with disability who received specialist disability services before the National Disability Insurance Scheme (NDIS) commenced in their region. Due to their age, these people were unable to transition to the NDIS. DSOA is a closed program and does not accept new participants.
80 Department of Health, Disability and Ageing, Budget 2024–25: Health and Aged Care Portfolio Budget Statements, DHDA, Canberra, 2024, available from https://www.health.gov.au/resources/publications /budget-2024-25-health-and-aged-care-portfolio-budget-statements?language=en [accessed 4 November 2025].
81 Two projects were in response to Fair Work Commission determinations in the Aged Care Work Value Case to increase award wages for aged care employees. One project was the CHSP client transition project.
82 The Aged Care Act 1997 defines the Aged Care Quality Standards as the standards for quality of care and quality of life for the provision of aged care. The Aged Care Quality Standards are set out in Schedule 2 of the Quality of Care Principles 2014.
83 The Serious Incident Response Scheme (SIRS) aims to reduce the risk of abuse and neglect of older people receiving aged care services. Providers are required to do everything reasonable and possible to prevent abuse and neglect of people receiving aged care services and act quickly to incidents, including allegations and suspicions. Providers are required to notify the ACQSC if particular incidents do occur. Provider obligations under the SIRS were implemented in the CHSP through provider grant agreements.
84 DHDA, CHSP Manual 2025–2027, 2025, pp. 8–9.
85 With the commencement of the Aged Care Act 2024, Commonwealth funded aged care services, including the CHSP, must be delivered by ‘registered’ providers. Providers are registered in one or more of six registration categories. The ACQSC is responsible for registering and monitoring providers, including auditing registered providers against the quality standards. Under the Aged Care Act 2024, assurance activities can include how registered providers use grants, charge for services and deliver aged care services.
86 The Home Care Packages Program assurance framework identifies four key program risks: people cannot exercise choice and control; the program does not achieve value for money; program funds are inappropriately or inadvertently used by providers; and program funds are fraudulently used by providers or care recipients.
87 DHDA’s Assurance Framework defines assurance confidence as ‘The level of faith a person has in the accuracy of the information they rely upon. Greater assurance confidence comes from forms of assurance that are provided independent of the function, follow a rigorous methodology, are explanatory in their presentation and are timely.’
88 The data quality statement explained this could be due to: lack of clarity in relation to data to be captured and reported by service providers, including ambiguous or poorly defined criteria, or mandatory data requirements not adequately defined; lack of education and awareness with respect to data reporting requirements; lack of system controls (e.g. mandatory/smart fields) to promote accurate completion of requisite data fields; no requirement for providers to confirm data is accurate and complete; or issues with transmission/upload of data from service provider systems to DEX.
89 The data quality statement explained this could be due to providers creating fictitious clients or intentionally reporting inaccurate results.
90 The Aged Care Quality Indicator Program has 11 measures that residential aged care providers are required to report on every three months. In 2024, DHDA consulted with aged care stakeholders on the development of quality indicators for the Support at Home program.
91 At the end of the 2023 Q1 review DHDA undertook a lessons learnt workshop to identify what worked well in 2023 and what could be improved for the 2024 process. Improvement opportunities included internal arrangements, provider communication and information to be requested from providers.
92 Under the Aged Care Act 2024, the Secretary of DHDA is the aged care System Governor, whose role includes: facilitating equitable access to aged care services; providing stewardship of the administration of aged care; and protecting and upholding the integrity of the administration of the aged care system and the Commonwealth’s investment in the system. ACQSC is the national regulator of aged care services.
93 This audit did not assess the ACQSC’s exercise of its assurance functions.
94 Excludes requirements under legal frameworks outside of aged care (for example, work health and safety requirements).
95 The eight Aged Care Quality Standards were: Standard 1 — consumer dignity and choice; Standard 2 — Ongoing assessment planning with consumers; Standard 3 — Personal care and clinical care; Standard 4 — Services and supports for daily living; Standard 5 — Organisation’s service environment; Standard 6 — Feedback and complaints; Standard 7 — Human resources; Standard 8 — Organisational governance. The standards changed under the Aged Care Act 2024.
96 Department of Health, Disability and Ageing, Commonwealth Home Support Manual - 2025-27, DHDA, Canberra, 2025, Appendix G, available from https://www.health.gov.au/node/56679 [accessed 14 April 2026].
97 Older Persons Advocacy Network, Presenting Issues, OPAN, Canberra, available from https://opan.org.au/information/publications-and-reports/reports/ [accessed 3 November 2025].
98 The ACQSC publishes quarterly sector performance reports that includes complaints data for CHSP. For 2024–25 the rate of complaints for the CHSP ranged from 1.4 to 1.7 per 10,000 consumers. For the Home Care Packages Program, the rate of complaints for 2024–25 ranged from 32.7 to 35.2 per 10,000 consumers.
Aged Care Quality and Safety Commission, ACQSC sector performance report quarter 4 (April – June 2025) Summary data tables, ACQSC, available from https://www.agedcarequality.gov.au/news-publications/reports/sector-performance [accessed 13 February 2026].
99 Aged Care Act 2024, section 5, available from https://www.legislation.gov.au/C2024A00104/latest/text [accessed 28 October 2025].
100 The Treasury, What is evaluation?, Treasury, Canberra, 2023, available from https://evaluation.treasury.gov.au/toolkit/what-evaluation#s5 [accessed 3 November 2025].
101 Public Governance, Performance and Accountability Act 2013, Section 39, available from https://www.legislation.gov.au/C2013A00123/latest/text [accessed 5 November 2025].
102 Department of Finance, Developing performance measures (RMG 131), Finance, Canberra, 2025, available from https://www.finance.gov.au/government/managing-commonwealth-resources/developing-performance-measures-rmg--131 [accessed 19 September 2025].
103 Department of Health, Disability and Ageing, Corporate Plan 2025–26, DHDA, Canberra, 2025, p. 99, available from https://www.health.gov.au/about-us/corporate-reporting/corporate-plan [accessed 4 November 2025].
104 Auditor-General Report No. 25 2024–25, Performance Statements Auditing in the Commonwealth — Outcomes from the 2023–24 Audit Program, ANAO, Canberra, Appendix 1, available from https://www.anao.gov.au/work /performance-statements-audit/performance-statements-auditing-the-commonwealth-outcomes-from-the-2023-24-audit-program [accessed 31 October 2025].
105 ibid.
The CHSP performance measure relies on provider reporting into the Data Exchange (DEX) system, which is placed into the Aged Care Data Warehouse by the Department of Social Services Community Grants Hub.
106 Department of Health, Disability and Ageing, Corporate Plan 2025–26, DHDA, Canberra, 2025, p. 99, note 93, available from https://www.health.gov.au/about-us/corporate-reporting/corporate-plan [accessed 4 November 2025].
107 The dashboard notes that numbers for demographic sub-groups may not be consistent with actual numbers due to a data characteristic.
108 DHDA advised the ANAO in September 2025 that the CHSP is not identified as a ‘program’ under which individual projects would be nested in its project management system, Altus.
109 The Australian Government does not have a preferred CHSP Goods Equipment and Assistive Technology (GEAT) provider. The government funded 89 equipment providers in 2024–25, including GEAT2GO to meet the equipment needs of older people across Australia. GEAT2GO (operated by Indigo Australasia) is contracted to trial a national service delivery model and supply items to CHSP clients alongside other CHSP equipment providers. GEAT2GO is intended to be a provider of last resort to meet the overflow demands for items the clients local CHSP provider cannot meet.
110 The Treasury, Commonwealth Evaluation Toolkit [Internet], Treasury, Canberra, 2023, available from https://evaluation.treasury.gov.au/toolkit/commonwealth-evaluation-toolkit [accessed 3 November 2025].
111 AusTender contract notice CN3964852, Callida Consulting, published 11 May 2023, contract value $452,764 at date of execution.
112 AusTender contract notice CN3841159, Health Policy Analysis, published 13 January 2022, contract value $629,200 at date of execution.
113 AusTender contract notice CN3575846, Australian Healthcare Associates, published 7 March 2019, maximum contract value $2,723,473 at date of execution.
114 AusTender contract notice CN3703052, Deloitte, published 21 July 2020, maximum contract value $200,000 at date of execution.
115 AusTender contract notice CN3786241, ACIL Allen Pty Ltd, published 25 June 2021, maximum contract value $300,000 at date of execution.
116 AusTender contract notice CN3964852, Callida Consulting, published 11 May 2023, contract value $452,764 at date of execution.
117 The Royal Commission examined variations in the CHSP service types and access across states and territories and other geographic factors and considered the National Ageing Research Institute’s survey findings on people’s experiences of aged care which included CHSP respite care clients.
118 Australian Public Service Commission, Capability Review: Department of Health and Aged Care, APSC, Canberra, 2023, pp. 19, 24, 28, 41–42, available from https://www.apsc.gov.au/initiatives-and-programs/workforce-information/research-analysis-and-publications/capability-review-department-health-and-aged-care [accessed 4 November 2025].
119 The National Aged Care Mandatory Quality Indicator Program collects information from Australian Government-funded residential aged care homes on 14 quality indicators across critical areas of care that can affect the health and wellbeing of aged care home residents. The program is designed to help monitor and improve the quality of services.
120 Mental health conditions included mood disorders, anxiety and/or stress disorders, and psychotic disorders.
121 The ANAO cross-referenced the names of the organisations provided by survey participants against Australian Business Numbers (ABNs). Four names were unable to be cross matched to an ABN and are not represented among the 436 providers or in response rate calculation.
122 There was a full enumeration of email addresses for Indigenous persons and balancing on the basis of available demographic information.
123 The reserve and boost samples did not receive the pre-notification email.
124 SEIFA refers to the Australian Bureau of Statistic’s Socio-Economic Indexes for Areas and the IRSD stands for the Index of Relative Socio-economic Disadvantage. These are derived from postcode.